
Common Misconceptions About the Clinical Use of HiTOP
A Guest Post by Whitney Ringwald

Whitney Ringwald is a doctoral candidate in the department of clinical psychology at the University of Pittsburgh and has a master’s degree in social work. Her research focuses on linkages between personality and psychopathology, and how their intersection can help us understand the whole spectrum of psychological functioning. You can learn more about her work on her website here and you can find her on twitter @WhitneyRingwald.
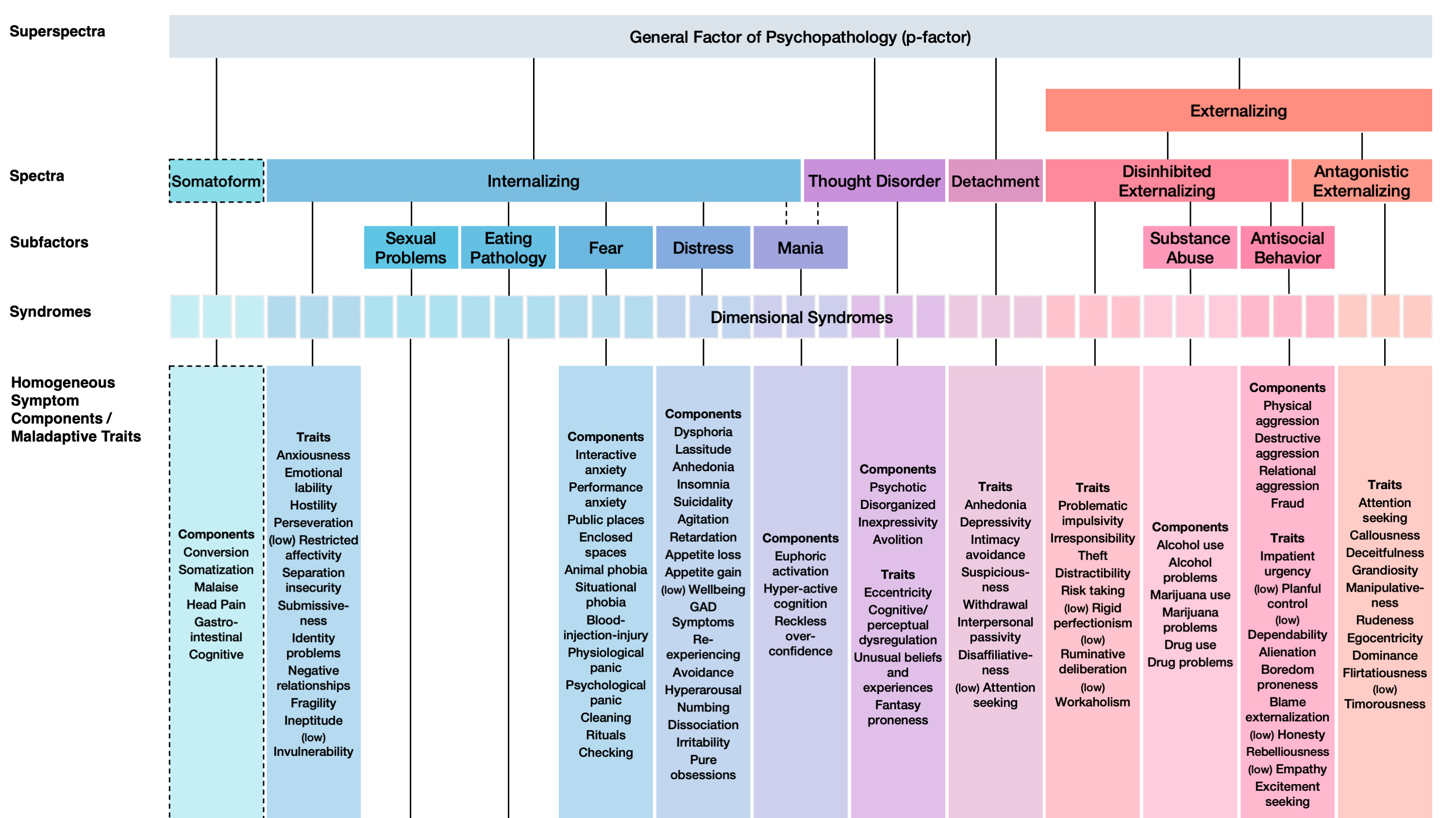
The Hierarchical Taxonomy of Psychopathology (HiTOP) is an empirically based, quantitative nosology of mental disorders. HiTOP was developed as an alternative to prevailing classification and diagnostic systems like the DSM. Instead of categorical diagnoses, the HiTOP system consists of hierarchically organized dimensions of psychopathology from specific signs and symptoms to increasingly broad constructs (e.g., internalizing/externalizing) encompassing features that cut across traditional disorders. This hierarchical, dimensional model is based on consensus from findings on the empirical psychometric structure of psychopathology. There is growing enthusiasm that HiTOP may be able to overcome problems with DSM diagnoses like extensive comorbidity, within-diagnosis heterogeneity, poor reliability, arbitrary thresholds, and preponderance of subthreshold and “not otherwise specified” cases.
Many mental health professionals see the merits of HiTOP for research. Many mental health professionals also acknowledge that DSM diagnoses have shortcomings in clinical practice. At the same time, a common refrain I hear from practitioners is that the DSM isn’t that bad; the diagnoses communicate clinical information pretty well, the polythetic criteria are easy to apply, and they provide decent coverage of most patients’ problems. We all know they aren’t intended to be applied rigidly; they’re more of a useful heuristic and match our intrinsic capacity for prototype matching. According to this line of thinking, the transition to a dimensional diagnostic system like HiTOP would require starting from scratch in some ways, which would be highly disruptive to day-to-day clinical operations, require lots of retraining for clinicians, and make decades of research and treatment development based on DSM diagnoses irrelevant (see, e.g., commentaries here, here, and here). So why throw the baby out with the bathwater? I think that these concerns are based on misconceptions about HiTOP.
HiTOP reorganizes signs and symptoms from DSM diagnoses into hierarchical dimensions, based on empirical covariation. Because of this, using HiTOP in clinical practice is radical in the sense that it’s a fundamentally different way of conceptualizing psychopathology, while at the same time it is conservative in that it retains all the clinical information mental health professionals know and rely on from the DSM and DSM-related research.
A core misconception to address up front is that HiTOP introduces entirely new diagnostic constructs. HiTOP doesn’t introduce new information per se, it just reorganizes signs and symptoms from DSM diagnoses into hierarchical dimensions, based on empirical covariation. Because of this, using HiTOP in clinical practice is radical in the sense that it’s a fundamentally different way of conceptualizing psychopathology, while at the same time it is conservative in that it retains all the clinical information mental health professionals know and rely on from the DSM and DSM-related research. Stemming from this core misconception are five specific misconceptions that I think fuel skepticism about HiTOP’s clinical utility:
1. HiTOP denies qualitative differences in normative and pathological functioning
As Jerome Wakefield eloquently pointed out, statistical extremity is an insufficient definition of dysfunction, and qualitative differences in functioning are central to the ontology of psychopathology for many clinicians. For example, those who have known someone in an acute psychotic state would have a hard time denying that they are having a categorically different experience of reality than someone who is just eccentric (i.e., slight elevation on the psychoticism dimension). To take another example, there is clearly a difference between someone who is introverted and someone who is pathologically socially withdrawn, even if they received the same score on the HiTOP dimension of detachment. While HiTOP describes this variability in terms of quantitative differences, it makes no assumptions about the underlying processes that distinguish normative and pathological functioning, and is therefore compatible with qualitative explanations of psychopathology. Thus, HiTOP serves as a theory-neutral framework for understanding qualitative variation rather than denying it.
HiTOP serves as a theory-neutral framework for understanding qualitative variation rather than denying it.
2. HiTOP dimensions do not fit with the categorical decisions in clinical practice
It is often argued that we need categorical thresholds because treatment decisions like whether to hospitalize, medicate, or discharge a patient are categorical. In practice, however, the cutoff on a single measure or diagnosis is rarely the sole basis for a treatment decision, and different cutoff points may be used for different points along a continuum of care (e.g., outpatient, intensive outpatient, partial, and inpatient). HiTOP provides diagnostic constructs that would allow for specifying thresholds along the distributions tailored to the range of clinical contexts and their decisions. In fact, efforts within HiTOP are currently underway to develop an omnibus measurement system with guidelines for tiered clinical cutoffs. Making clinical decisions within a HiTOP framework would therefore hardly be a departure from prevailing practices, and the dimensional, hierarchical structure would permit the formal instantiation of graded thresholds that are now often employed in an ad hoc manner.
3. You can’t make empirically based treatment selections with HiTOP constructs
Since medication trials typically test efficacy in samples of patients with a DSM diagnosis, and many psychotherapies are designed to treat a specific DSM disorder, a concern is that there will be no empirical guide for treating patients with a HiTOP-based diagnosis. This is not much of an issue since the direct crosswalk between DSM disorders/ICD codes and HiTOP dimensions makes it straightforward to translate diagnosis-specific evidence into a HiTOP framework. Perhaps more importantly, there’s already a mismatch between diagnoses and treatments when using the DSM, given that many patients have subthreshold symptoms or symptoms that cut across multiple diagnoses. As a result, patients with a wide array of clinical presentations get the same treatments and patients with the same diagnosis often get different treatments. HiTOP arguably makes bridging treatment research with a patient’s clinical presentation more systematic by providing constructs that describe higher-order features in common across patients with varying presentations that could make them responsive to the same treatment (e.g., negative emotionality and SSRIs) and lower-order features that may predict differential treatment response within the same diagnosis (e.g., emotional instability vs. anhedonia in depression).
4. HiTOP would make it more difficult to communicate clinical information to other mental health professionals and to patients
The argument goes that since clinicians and patients are more familiar with the DSM diagnoses than HiTOP constructs, the DSM is better for efficiently communicating a patient’s problems. One issue with this logic is that DSM diagnoses aren’t that informative due to within-diagnosis heterogeneity. It’s not really sufficient in most treatment coordination contexts to say a patient has Major Depressive Disorder, for example, because one has to clarify the particular symptom presentation to really know the nature of their problem (Anhedonia? Low mood? Increased appetite? Decreased appetite? Low energy? Irritability?), and to note other non-depressive symptoms (Anxiety? Personality pathology?). DSM diagnoses also don’t directly speak to the severity of a patient’s problems, or their global functioning, which is another critical piece of clinical information for treatment coordination. The hierarchical structure of HiTOP more directly captures these different levels of information than the DSM. With HiTOP, the complexity of symptom configuration can be described at the lower-order levels, while severity can be described by dimensions at the higher-order levels. HiTOP could therefore enhance the precision of clinical communication.
For communicating with patients, clinicians often have to “unpack” a heterogeneous DSM diagnosis by relating it to their more specific presenting problems. Also, most treatments consist of monitoring and targeting narrow symptoms rather than a diagnosis. What may be most important when it comes to communicating diagnostic information to a patient is that it helps them make sense of their experience and provides a clear path forward for treatment. As discussed at length elsewhere, the DSM falls short of this goal. Because HiTOP constructs can more flexibly describe a patient’s presenting problems than DSM diagnoses, it could allow patients to conceptualize their problems in a more personalized and meaningful way. And as noted above, since HiTOP is facilitative of treatment planning, it can provide the hope patients benefit from.
Because HiTOP constructs can more flexibly describe a patient’s presenting problems than DSM diagnoses, it could allow patients to conceptualize their problems in a more personalized and meaningful way.
5. Mental health professionals prefer the DSM and will be resistant to HiTOP
A concern that’s often raised is that even if HiTOP could be transformative, that potential won’t be realized if clinicians don’t embrace the change and put HiTOP into practice. That’s for sure; no argument there. And, it is reasonable to think that clinicians trained using the DSM would prefer to use that system rather than learn a new one, but results of several surveys of mental health professionals suggest this will not be a concern. In a recent study, it was found that practicing clinicians (predominantly clinical psychologists) preferred HiTOP over the DSM for formulating interventions, communicating clinical information, comprehensively describing psychopathology, and ease of application. What is particularly remarkable about these results is that this preference held for clinicians who’d never heard of HiTOP, suggesting it is a highly intuitive system. A few other studies (e.g., here, here, and here) have similarly shown that clinicians prefer dimensional measures of pathological personality traits akin to HiTOP over categorical personality disorder diagnoses on most indices of clinical utility. So, it seems like many mental health professionals would readily adopt HiTOP if given the chance.
In sum, HiTOP reorganizes clinical information from the DSM in a way that aligns more closely with how patients actually present and with how case conceptualization, communication, and decision-making are already conducted. Using HiTOP could help make clinical practice more effective and efficient. And likely because of the tighter alignment between the diagnostic model and clinical reality, there is evidence to expect that mental health professionals will pick up the new system with relative ease and may even prefer it over the DSM. So to those fretting over what will get thrown out in the transition to using HiTOP in clinical practice—don’t worry, the baby will be safe.
This is really helpful. I am very interested in learning more about HiTOP.