
Dexamethasone Suppression Test - The OG Psychiatric Biomarker
The clinical application of a well-replicated association remains unclear

The review article “Cortisol and the Dexamethasone Suppression Test as a Biomarker for Melancholic Depression: A Narrative Review” by Martin M. Schumacher and Jacopo Santambrogio stimulated my interest again in the Dexamethasone Suppression Test (DST) as a biomarker in psychiatry and led me down a rabbit hole of old and new research assessing its value. Like Schumacher and Santambrogio (S&S), I find myself grappling with the question of why DST, which was once an exciting and promising biomarker of melancholic depression and which has considerable empirical support, never led to meaningful clinical application.
The hypothalamic-pituitary-adrenal axis (HPA) is the body's main stress response system, and DST checks how well it is working. DST is classically used to diagnose Cushing’s disease/syndrome, a medical condition caused by prolonged exposure to excessive levels of the hormone cortisol or to other glucocorticoid hormones. The test checks how levels of cortisol change when dexamethasone, a synthetic glucocorticoid 25 times stronger than cortisol, is administered. If the HPA system is working properly, giving dexamethasone lowers the amount of cortisol in the body. This is because of activation of negative feedback mechanisms that control the HPA axis. Inadequate suppression of cortisol, or a reduction that is less than expected, is a sign that the negative feedback system is not working optimally.
In the psychiatric context, DST was proposed to be a marker for the melancholic or endogenous subtype of depression. “Endogenous” depression is an older term used for depressive states where the presentation suggests a biological etiology (a problematically speculative characterization, which is why the term is no longer in official use). “Melancholic” depression is characterized by features such as severe anhedonia (inability to experience interest or pleasure), lack of mood reactivity, loss of appetite, psychomotor agitation or retardation, and early morning awakening. The two terms were often used interchangeably prior to DSM-III.
In the classic 1981 article, Bernard Carroll et al. reported:
“Four hundred thirty-eight subjects underwent an overnight dexamethasone suppression test (DST) to standardize the test for the diagnosis of melancholia (endogenous depression). Abnormal plasma cortisol concentrations within 24 hours after dexamethasone administration occurred almost exclusively in melancholic patients. The best plasma cortisol criterion concentration, above which a DST result may be considered abnormal, was 5 ug/dL. The optimal dose of dexamethasone was 1 rather than 2 mg. Two blood samples obtained at 4 and 11 PM after dexamethasone administration detected 98% of the abnormal test results. This version of the DST identified melancholic patients with a sensitivity of 67% and a specificity of 96%. Baseline nocturnal plasma cortisol concentrations were not useful. Abnormal DST results were found with similar frequency among outpatients and inpatients with melancholia; but they were not related to age, sex, recent use of psychotropic drugs, or severity of depressive symptoms. Extensive evidence validates this practical test for the diagnosis of melancholia.” (my emphasis)
Research over the next decade produced results that were less striking, inconclusive, and even contradictory.
S&S write:
“This article was met with great interest and enthusiasm by the psychiatric community and triggered many studies by other researchers using the DST as a diagnostic tool in psychiatry. Unfortunately, the results of these studies were inconsistent and, for the most part, did not confirm Carroll’s findings and claims.”
And conclude from their discussion:
“The DST as proposed by Carroll et al. in 1981 was never fully developed, validated, or standardized. A plethora of investigations by other research groups applying the DST yielded contradictory findings, which resulted in it finally being rejected. In addition, many technical and political issues, diagnostic fuzziness, and the prevailing zeitgeist contributed to the fall from grace of this promising biomarker.”
S&S make a number of important suggestions regarding the standardization of the experimental parameters and incorporation of relevant factors, but they particularly focus on the need for diagnostic clarity when it comes to DST. “Major Depressive Disorder” is a broad and heterogenous category introduced in 1980 in DSM-III. DST is not sensitive or specific enough for depression as a whole, so relying on MDD ensures that DST would fail as a diagnostic biomarker.
“It must be emphasized that the current diagnostic concept of major depressive disorder (MDD) as found in the DSM-5-TR and ICD-11 should not be confused with melancholic depression. The DST was and is intended to be used only in cases of melancholia (in the broad sense of Kraepelin’s manic-depressive insanity). We emphasize the fact that the DST should be applied only to patients with the psychopathological picture of a severe depression in a broad sense (including psychotic depression, bipolar disorder, and schizoaffective disorder).” (my emphasis)
I think S&S are correct to highlight this, but I am nonetheless uncertain that DST can ever be of sufficient value as a marker to diagnose melancholic states. We can diagnose melancholic states clinically, and DST is unlikely to be superior to clinical judgment for this purpose. In fact, I am inclined to think that DST has failed as a biomarker because we have been so intent on studying it as a diagnostic biomarker. We might have more success if we look at it as a transdiagnostic marker of (sub-Cushingoid) HPA axis dysregulation, which is associated with different psychiatric syndromes to different degrees. We can then ask better questions about its clinical and etiological significance.
DST failed as a biomarker because the field was intent on studying it as a diagnostic biomarker. It might have succeeded if we looked at it as a transdiagnostic marker of (sub-Cushingoid) HPA axis dysregulation, associated with different psychiatric syndromes to different degrees. We could then ask better questions about its clinical and etiological significance.
In this post, I offer my assessment of the scientific literature on DST and psychopathology.
Does the association between (melancholic) depression and DST non-suppression hold up?
As far as I can tell, almost every review that has examined this question has concluded that yes, the association is genuine.
2018 systematic review: “Among the studies included in this systematic review that evaluated patients with melancholic depression, most (n=17) studies focused on DST response. Of them, the vast majority did indicate significantly elevated degrees of non-suppression in melancholic patients.”
Nestor L. Lopez-Duran, et al, 2009, meta-analysis in depressed children and adolescents:
We examined: (a) 17 published studies of HPA-axis response to the dexamethasone suppression test (DST) in depressed youth (DST; N = 926) and (b) 17 studies of basal HPA-axis functioning (N = 1332). We also examined descriptively studies that used corticotropin-releasing hormone (CRH) infusion, and those that used psychological probes of the HPA-axis. The global standardized mean effect size difference in HPA-axis response to the DST between depressed and non-depressed youth was 0.57, z = 4.18, p < 0.01. The global standardized mean difference effect size in basal HPA-axis functioning was 0.20, z = 4.53, p < 0.01. Age, sex, timing of sampling, dexamethasone dosage, or type of control group was not a significant source of variability for the DST or basal studies. In addition, when compared to non-depressed peers, depressed youth have a normative response to CRH infusion but an overactive response to psychological stressors.
Rush et al. 1996 study:
METHOD: 487 consecutive adult inpatients (N = 131) and outpatients (N = 356) with unipolar (N = 422) or bipolar disorder (N = 65) underwent the 1.0-mg DST. Nonsuppression was defined as at least one post-dexamethasone cortisol measurement > 4.0 µg/dL.
RESULTS: Nonsuppression occurred in 27% of all patients with major depression and 43% of all bipolar depressed phase patients. For outpatients, dexamethasone nonsuppression occurred in 35.2% of subjects with endogenous (unipolar + bipolar; N = 145) and 9.0% of those with nonendogenous (unipolar only; N = 211) depressions (single 4 p.m. post-dexamethasone cortisol). For inpatients, dexamethasone nonsuppression was found in 61.5% of subjects with endogenous (N = 104) and 18.5% of those with nonendogenous (N = 27) depressions (three postdexamethasone cortisol determinations). For the inpatient and outpatient sample together, the DST had a sensitivity of 46.2% and a specificity of 89.9% in differentiating endogenous from nonendogenous major depressive episodes. Weight loss, gender, and symptom severity added little to the endogenous/ nonendogenous dichotomy.
The association even shows up in a large population-based study with a non-psychiatric sample (N = 1822) using a very low dose DST: “Even though there were no linear associations between psychiatric measures and cortisol suppression, we found that depressive symptoms and anxiety disorders were more common in persons with non-suppression of cortisol. Conversely, psychotropic medication use was related to enhanced suppression of cortisol after DST.”
Research consistently points towards an association between depression and non-suppression on DST. This association is relatively more specific for depression with melancholic or psychotic features, and depression that leads to inpatient psychiatric hospitalization. But it is not sensitive or specific enough to serve as a substitute for clinical diagnosis.
How often do we see DST non-suppression in other psychiatric disorders?
Often enough.
The 2023 paper by S&S has two very useful tables to answer this. (They adapted the tables from Evans and Nemeroff 1987 and Murphy 1991.)


These tables also make a convincing case for not restricting DST to melancholic depression. We should be curious about the role HPA axis dysregulation is playing in psychopathology even when the individual has a clinical diagnosis of a diagnosis other than melancholia, such as anxiety, mania, or schizophrenia. There certainly appears to be a stronger association of DST non-suppression with melancholic, bipolar, and psychotic depressions (does DST non-suppression shift the symptom network towards the melancholic somehow?), but we shouldn’t assume that DST non-suppression is clinically meaningful only for these states.
Does DST non-suppression predict which depression treatment a person will respond to?
Even in the 1980s, the scientific answer to this question was… No.
Here are Gitlin and Gerner (1986) on DST and treatment response:
“The dexamethasone suppression test (DST) has been primarily investigated as an aid in diagnosing endogenous depression; yet, its major clinical use has been as a predictor of treatment response. It is commonly held that 1) an abnormal DST predicts response to somatic (and not psychologic) therapies, 2) an abnormal DST predicts response to noradrenergic antidepressants, and 3) a normal DST predicts response to serotonergic agents. The DST predicted response to somatic therapies in only 6 of 16 published studies. No single methodologic factor, such as population variables, DST technique, or study design, can explain the marked discrepancy in study results. Only two of seven studies examining the DST and response to neurotransmitter-specific antidepressant groups found a positive relationship. The evidence that the DST predicts response to noradrenergic agents is weak. The DST does not predict acute response to somatic treatment in general or response to specific antidepressants. The selection of the appropriate treatment for depressed patients is still best made using clinical criteria.”
In a trial reported in 1988, DST was not superior to a clinical judgment of “endogeneity” in predicting response to antidepressant treatment.
Research studies do seem to show that response to dexamethasone normalizes with remission (this is seen even with treatments such as TMS) and failure to normalize indicates a poorer prognosis.
Does DST non-suppression predict a response to placebo?
I can’t tell if this question has been systemically studied, but the research that I’ve come across does seem to consistently show that DST non-suppression is associated with a reduced response to placebo and reduced chances of spontaneous remission.
“Thirteen of 20 (65%) persistent depressives displayed positive DST results, whereas none of the placebo responders had an abnormal result…” (Zammit, et al. 1988)
Peselow et al, 1989: “The presence of a positive or negative DST did not predict response to either paroxetine or imipramine. However, a positive DST predicted a poorer response to placebo: only 3 out of 18 patients who showed DST non-suppression responded to placebo, as opposed to 11 out of 21 who exhibited DST suppression (P<0.05). A positive DST was associated with a 61% response to drugs and a 16% response to placebo. This finding suggests that the presence of a positive DST implies the need for active somatic treatment.”
Peselow et al, 1986: “In all, 68 patients required this trial, 31 receiving amitriptyline and 37 receiving desipramine. For these patients there was no relationship between DST suppression/non-suppression vs clinical response to either desipramine or amitriptyline. There was a non-significant trend for suppressors (negative DST) to respond either spontaneously or to low-dose desipramine or amitriptyline as opposed to non-suppressors (positive DST).”
Peselow et al, 1986: “… 61 depressed inpatients randomized to either one of two drugs, sertraline of oxaprotiline, or placebo over a 4-week clinical trial. For 30 patients who completed at least 3 weeks of double-blind treatment on either drug, the initial DST was not predictive of response to drug treatment. For the 17 patients who completed at least 3 weeks of double-blind treatment on placebo, the presence of a positive DST predicted a statistically significantly poorer response to placebo as opposed to a negative DST.”
If DST non-suppression does predict a poor response to placebo in depression, as it seems to, this could be particularly useful in clinical trials where high rates of response in the placebo arm make it difficult to demonstrate the effect of interventions. Why hasn’t this strategy already been employed, especially by pharmaceutical companies? I’m not sure, but this appears worth studying further.
If DST non-suppression does predict a poor response to placebo in depression, as it seems to, this could be particularly useful in clinical trials where high rates of response in the placebo arm make it difficult to demonstrate the effect of interventions. Why hasn’t this strategy already been employed, especially by pharmaceutical companies? I’m not sure, but this appears worth studying.
Ok, so melancholic depressions often show DST non-suppression… are there psychiatric disorders where individuals show DST hyper-suppression?
Actually, yes. DST hyper-suppression appears to be a fairly consistent finding in the context of psychiatric sequelae of trauma.
An extensive 2009 review by Kathryn Handwerger concluded:
“While PTSD and MDD share numerous overlapping symptoms, their HPA profiles are often strikingly different. Individuals with MDD often display heightened basal cortisol, DST nonsuppression, and either normal or slightly blunted cortisol increases in response to stress. By contrast, individuals with PTSD often display the opposite pattern: lower basal cortisol, hypersuppression in response to the (low dose) DST, and higher cortisol in response to stress. Despite the variability in this literature, the DST has produced the most consistent findings…”
However, subsequent research has shown that DST profiles do not discriminate between PTSD and MDD per se (MDD, as we noted, is a very heterogenous category). What seems to matter instead is the history of (childhood) trauma and abuse. Even depressed patients with a history of childhood trauma tend to show cortisol hyper-suppression on DST instead of non-suppression that characterizes melancholic depression.
Savic, et al. 2012 demonstrated that trauma-related psychopathology, whether depression or PTSD, shows the same pattern of hyper-suppression. Their study had 399 male participants: 57 with PTSD, 28 with depression, 76 with PTSD + depression, and 238 healthy controls. PTSD, depression, and PTSD+depression, all three suppressed cortisol after dexamethasone significantly more than healthy controls. “When the number of traumas was introduced as a covariate, the differences disappeared. The hypothesis was confirmed: in respect to DST, the examined trauma-related psychopathologies showed the same pattern: hypersuppression, due to multiple traumatic experiences.”
Newport, et al, 2004. showed that DST hyper-suppression isn’t strictly related to trauma history but is instead related to trauma-related psychopathology:
Methods: Standard and low-dose dexamethasone suppression tests (DST) were performed in women with a history of child abuse (n = 19), child abuse and major depression (n = 16), major depression and no childhood trauma (n = 10), and no history of mental illness or childhood trauma (n = 19). Secondary analysis with posttraumatic stress disorder (PTSD) as the organizing diagnosis was also conducted.
Results: In the low-dose DST, depressed women with a history of abuse exhibited greater cortisol suppression than any comparator group and greater corticotropin suppression than healthy volunteers or nondepressed abuse survivors. There were no differences between nondepressed abuse survivors and healthy volunteers in the low-dose DST or between any subject groups in the standard DST. The PTSD analysis produced similar results.
Conclusions: Cortisol supersuppression is evident in psychiatrically ill trauma survivors, but not in nondepressed abuse survivors, indicating that enhanced glucocorticoid feedback is not an invariable consequence of childhood trauma but is more related to the resultant psychiatric illness in traumatized individuals.
In another study, patients with borderline personality disorder and comorbid PTSD showed more pronounced cortisol suppression compared to those with BPD without PTSD, and these findings were stable over a follow-up period of one-year. (Wingenfeld, 2007)
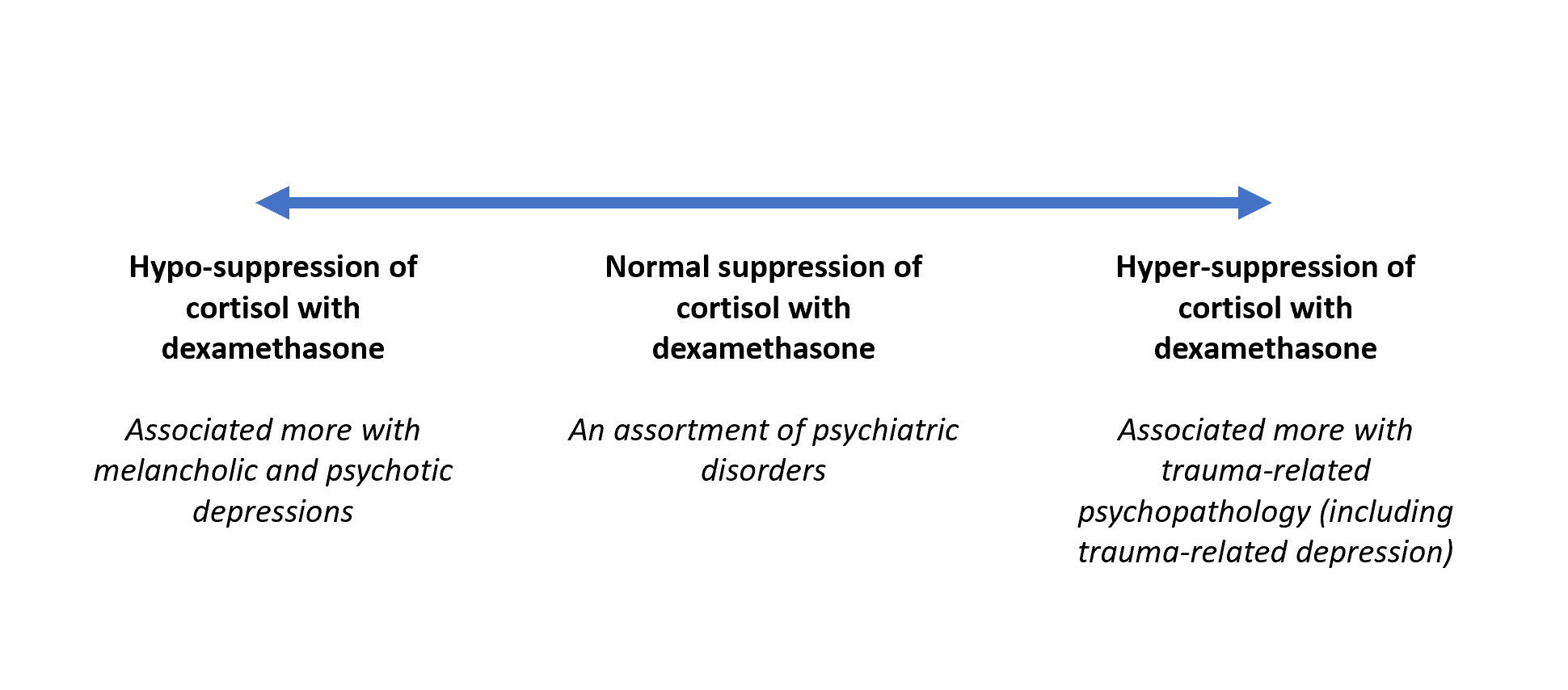
From the HPA axis perspective, it appears as if psychiatric conditions lie on a spectrum of varying degrees of hypo-suppression and hyper-suppression of cortisol to the administration of dexamethasone, with melancholic/psychotic depressions enriched at the hypo-suppression end and trauma-related psychopathology (including trauma-related MDD) at the hyper-suppression end.
Does DST non-suppression mean that HPA axis dysfunction is the primary pathology in these cases?
It’s hard to say. HPA axis dysfunction appears to be a part of the etiological picture, but we don’t know yet what the correct causal explanation is. The matter is certainly not as clear-cut as Cushing’s disease. HPA axis dysfunction of the degree seen in melancholic depression may simply be a sign of the illness, a sign among other signs such as psychomotor retardation and no more privileged as a window into pathophysiology, or it may point towards something more fundamental about causal mechanisms. Braddock made a similar point very well in 1986.
“… there is not so far any evidence for a pathological process occurring in endogenous depression, for which non-suppression is a marker. The test merely represents a statistical abnormality, related to the presence of illness, whose significance for the patient remains unclear.”
“The ability to measure precisely plasma hormone levels encourages the belief that neuroendocrine tests are thereby more fundamental and somehow nearer the putative neurophysiological abnormality than less precisely quantified behavioural or cognitive variables… Perhaps we should regard abnormal plasma cortisol control as just another symptom, like sleep disturbance, but one which we are fortunate enough to be able to subject to a dynamic test with an easily measured end-point. Just as with other symptoms of endogenous depression, the question whether non-suppression is a manifestation of supposed underlying pathology or is a secondary phenomenon, remains undecided by the evidence so far.”
It is unfortunate that decades later, we are still not in a position to answer this question. However, the fact that the hypo-suppressive and hyper-suppressive profiles align, albeit imperfectly, with the melancholic and traumatic clinical profiles suggests to me that the HPA axis may be an important mechanism connecting etiological factors to clinical symptomatology.
Comments are open.
I’m posting this comment on behalf of Martin Schumacher (first author of the 2023 review article I linked above):
“I enjoyed reading this blog about the DST as a biomarker in psychiatry. Indeed, its usefulness as a diagnostic biomarker of melancholic depression (MD) is limited, as MD can be clinically diagnosed (e.g., by using the sign-based CORE criteria developed by Gordon Parker). But even in this situation, the DST could serve as a valuable test to substantiate/confirm the clinical diagnosis.
Other potential clinical uses of the DST are the assessment of the risk of suicide and the success of treatment (with ECT, TCAs or MAOIs). A response to treatment which is not accompanied by a normalization of the DST is likely to be followed by a relapse. The most important application of the DST is probably in drug development. Here, the DST will help to identify biologically homogenous patient groups.
As Aftab suggests, the DST should be applied in a transdiagnostic manner. The artificial borders between DSM-based diagnostic entities are very porous or even flatly wrong. The “manic-depressive insanity” diagnostic entity of Kraepelin (i.e., severe recurrent depression and/or mania, and psychosis) should be the main target of the DST.
I am not familiar with the literature about the DST and trauma and/or PTSD. However, this looks like another interesting field of application.
The outcome of the DST should not be interpreted in a strict binary fashion (i.e., suppression vs non-suppression), but as a continuous output. This continuum covers non-suppression (i.e., no suppression at all) all the way to a total suppression of cortisol secretion.
In this context, the fact that both Cushing's disease (hypercortisolism) and Addison's disease (hypocortisolism) are associated with depression and/or psychosis is noteworthy. Besides the DST, also the level and the shape of a cortisol diurnal profile might add useful information.
The DST assesses (only) the functionality of the HPA-axis. We should not forget that disturbances of all other endocrine axes are also related to psychiatric symptoms.
More information about these subjects can be found here:
https://inhn.org/inhn-projects/controversies/default-title
“
Does DST non-suppression predict a response to a controlled increase in exercise combined with a ketogenic diet and regulation of the circadian rhythms? I’ve seen that folks who seem to present with an “endogenous depression” or bipolar spectrum picture - where the changes in mood seem unrelated to psychological meaning making tend to respond more to well formulated and supported lifestyle medicine (diet, sleep, exercise) as a primary treatment target.