
Polygenic Embryo Screening and Schizophrenia Risk Reduction

I have been mulling over a theoretical issue pertaining to polygenic embryo screening for schizophrenia. It is recognized by practically everyone in behavioral genetics that the polygenic risk score (PRS) for schizophrenia currently captures only a small variance of the risk for the disorder. Schizophrenia PRS explains approximately 8% of the variance in risk in independent samples. Yet, under certain assumptions, polygenic embryo screening based on schizophrenia PRS can lead to relative risk reductions as high as 50%! How come? This post is my attempt to make sense of this relative risk reduction and place it in the appropriate scientific context. A focus on 50% relative risk reduction glosses over many important details, and the actual risk reduction we may expect in the real world is substantially lower and uncertain.
First things first… what even is polygenic embryo screening based on polygenic risk score?
Single-nucleotide polymorphisms (SNPs) are small differences in DNA sequence that vary from person to person. Each SNP might slightly alter the risk of developing common diseases. However, since one SNP alone usually has a minimal impact, multiple SNPs and their effect sizes can be added together in the form of a polygenic risk score (PRS) to allow for an estimate of the individual’s disease risk. SNPs are identified using large genome-wide association studies (GWASs). GWAS involves scanning genetic markers across the complete sets of DNA of a large number of people to identify genetic variations (SNPs) associated with a particular disease or trait.
Preimplantation genetic testing during in-vitro fertilization (IVF) has been commonly employed for decades now. It allows the identification of specific genetic disorders in embryos before they are implanted. It’s especially helpful in the case of serious genetic diseases such as cystic fibrosis or Tay-Sachs disease. Parents can choose to implant embryos that don’t carry these harmful genes. GWAS has opened up broader possibilities for preimplantation genetic testing. Now, we can analyze the genetic makeup of cells from an embryo to predict the likelihood of more common and complex conditions, including various psychiatric disorders as well as traits such as height or intelligence. This is known as polygenic embryo screening (PES). Genetic material from each embryo during an IVF cycle is analyzed, and polygenic scores for various conditions are calculated. Based on these scores, prospective parents can decide which embryos to implant.
Polygenic embryo screening is already commercially available. It is, however, controversial. The general opinion in the medical and genetics communities is that polygenic embryo screening isn’t ready for routine clinical use. The International Society of Psychiatric Genetics issued a statement in 2021 saying that the accuracy of PRS in psychiatry is not sufficient for clinical use, urging “caution” and calling for “additional research and oversight on the use of polygenic embryo screening.” Folks from the European Society of Human Genetics called polygenic embryo screening “an unproven, unethical practice” in 2021, Polyakov et al. (2022) said it is “not ready for prime time," and Johnston & Matthews (2022) wrote in Nature Medicine that the clinical utility is “unclear” and “profound ethical implications” need a “frank assessment.” In a survey of experts in psychiatric genetics published in 2023, more than 60% of experts were of the view that no clinical uses of PRS for schizophrenia are appropriate at present (although the vast majority thought that clinical use would be appropriate in 10 years). Some people feel differently about PES, of course. I am not here to argue either way. In the absence of a strong and qualified opinion of my own, I will defer to the expert consensus. (For a different view, see Scott Alexander’s discussion of polygenic selection here and here.)
For my discussion of schizophrenia, I am using two sources for the estimates of reductions in relative risk. The first is a 2021 paper by Lencz et al in eLife, in which they examine the use of polygenic embryo screening by simulating ‘virtual’ couples and offspring based on real genomes from schizophrenia case-control studies. They consider 2 different types of embryo selection strategies: high risk exclusion and lowest risk prioritization. In the high-risk exclusion strategy, embryos with extremely high PRS for the condition (e.g., in the top 2 percentile) are excluded, and an embryo is randomly selected from the remaining. Lencz et al. show that a high risk exclusion strategy produces small relative risk reductions, often less than 10%. In the lowest risk prioritization strategy, the embryo with the lowest disease PRS is selected, and Lencz et al. show that theoretical risk reduction using lowest risk prioritization can be quite large. For schizophrenia, their model shows that a relative risk reduction of up to 52% is attainable when selecting from 5 available embryos using the lowest risk prioritization strategy. This is despite the fact, as they themselves acknowledge, that the PRS accounts for only about 8% of the variance in liability.
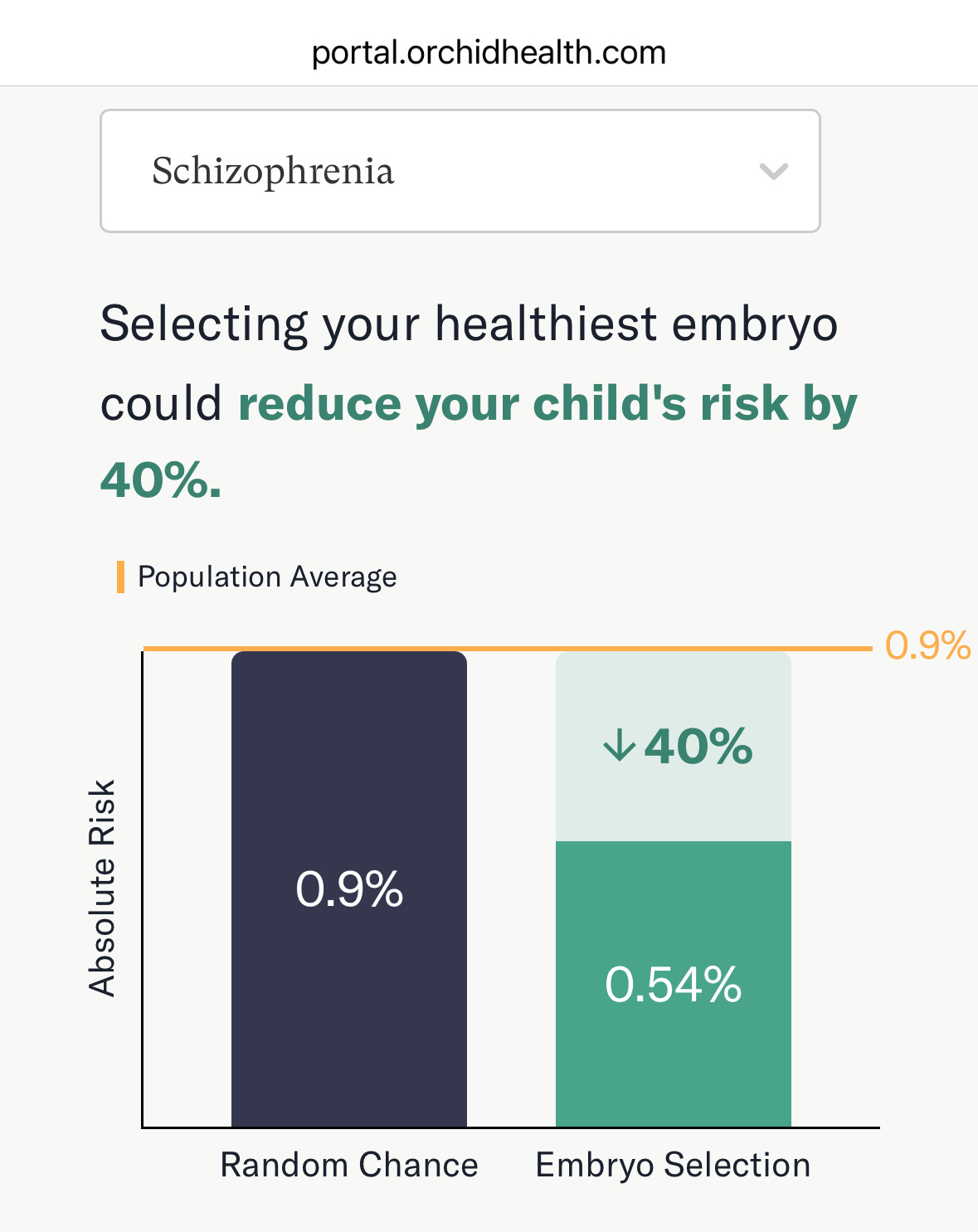
My second source is the online risk calculator on Orchid Health’s website, a company offering polygenic embryo screening commercially. They use the lowest risk prioritization strategy and offer similarly high relative risk reduction estimates, 50% relative risk reduction for someone without a family history of schizophrenia (50% reduction if population prevalence is taken to be 1%; 40% reduction if it is taken to be 0.9%, which is what their risk calculator shows).
In the rest of this post, my goal is to unpack these estimates, explain how we arrive at these numbers, and explain how our assessment of these numbers may change once we take the overall context and other scientific details into account.
For disorder categories with a threshold character, even a small shift in underlying vulnerability can produce large changes in the proportion of affected individuals.
Lencz et al. (2021) explain:
“While our prior work (Karavani et al., 2019) demonstrated that PES would have a small effect on quantitative traits, here we show that a small reduction in the liability can lead to a large reduction in the proportion of affected individuals. This is fundamentally a property of a threshold character with an underlying normally distributed continuous liability. For such traits, most of the individuals in the extreme of the liability distribution (i.e. the ones affected) are concentrated very near the threshold. Thus, even slightly reducing their liability can move a large proportion of affected individuals below the disease threshold. However, it should be noted that conventional thresholds for defining presence of disease may contain some degree of arbitrariness if the underlying distribution of pathophysiology is truly continuous. Consequently, the effects on ultimate morbidity may depend on the validity of the threshold itself (Davidson and Kahn, 2016).”
A large relative risk reduction may nonetheless mean a small absolute risk reduction.
Absolute risk reduction is defined as the difference between the baseline disease risk and the risk following either strategy of embryo selection. Since schizophrenia is an uncommon condition with a baseline population rate of about 1%, a 50% decrease in risk translates to an absolute reduction of 0.5%. As Lencz et al. (2021) put it:
“a randomly-selected embryo would have a 99% chance of not developing schizophrenia, compared to a 99.5% chance for an embryo selected according to LRP.”
For any particular individual who is already at low risk of schizophrenia, this decrease in risk is not worth undertaking IVF and PES just for the purpose of reducing schizophrenia risk. And if someone were undertaking IVF and PES for other purposes, they would likely have reasons to prioritize the risk of other medical conditions over the already low risk of schizophrenia.
This is why Turley et al. (2021) in a special report for the New England Journal of Medicine recommend emphasizing absolute risk reduction over relative risk reduction in PES:
“absolute risk reduction should be the most salient measure of expected gain in tables, figures, and other materials. Relative risk reduction associated with embryo selection based on polygenic scores should never be presented in isolation.”
(I do want to acknowledge here, theoretically speaking — and this is more of a speculative sci-fi scenario at present — if we ever got to a point where most births were taking place after IVF and PES, a 40-50% reduction in schizophrenia risk at the population level would certainly be huge.)
There are uncertainties around the predictive value of polygenic risk scores.
Orchid’s predictions for schizophrenia are based on data from the UK Biobank. The following figure from the Orchid Schizophrenia whitepaper shows the relationship between PRS and schizophrenia prevalence. (Genetic Risk Score here is the same as Polygenic Risk Score). Even though schizophrenia PRS accounts for 8% of risk variability, we can see that it correlates with schizophrenia prevalence in the sample. People with a higher PRS are at a higher risk of schizophrenia. The predictive power of schizophrenia PRS extends beyond the individual effects of the identified SNPs in the PRS score. We have only identified a fraction of the genes associated with schizophrenia, but it is likely that a person with a high PRS for schizophrenia also has a greater number of unidentified genetic variants associated with schizophrenia. PRS is therefore an imperfect marker of overall genetic risk.

Since the predictive power of PRS depends on many unknown associations, there is inherent uncertainty when generalizing predictions from one population sample to another sample or to an individual. Some factors to take into account include differences in ancestry, differences in demographics (such as socioeconomic status), confounding effects of genetic nurture, and clarity of phenotypic definitions.
Lencz et al. (2022) in a paper for Lancet Psychiatry explain this quite well:
“Given the minute effect sizes of individual alleles in a given GWAS, which are sensitive to many potential sources of artifact, the accuracy of a PRS is a function of both the size of the GWAS and its similarity to the target individual. The predictive accuracy of PRS is therefore reduced when applied to individuals from populations that differ from the original GWAS population. This is an important concern, since most current GWASs use samples of convenience to obtain the large sample sizes required for statistical power, and therefore a given embryo might not resemble the types of people included in the GWAS. For example, one well-known and widely discussed limitation is the problem of PRS portability across individuals of different ancestries. Allele frequencies and linkage disequilibrium structures tagging the contributory variants differ due to different demographic histories. To date, the large majority of GWASs include only populations of European descent, and people with African ancestry are particularly understudied. In the context of PES, the attainable risk reductions for embryos of African ancestry are only about half of those available for those of European ancestry across a range of diseases and traits (including intellectual disability). Moreover, recent studies have shown that PRSs might differ systematically in subpopulations of the same continental ancestry, if they vary even slightly from the original discovery sample. These effects are driven not only by differences in allele frequencies and linkage disequilibrium due to drift, but also by recent events in demographic history (such as urbanisation or recent admixture), that might affect genotype–phenotype relationships. Although several promising techniques to enhance portability across ancestries are under development, the genetics of common disease could be sufficiently complex that any proposed statistical adjustments will have fundamental limitations to their ability to translate PRSs from one population to another. Thus, clinical applications of PRSs, including in the IVF setting, could increase the inequities that already plague health-care delivery.
More broadly, accuracy of a PRS depends on various factors that might differ between the training GWAS and the population to be estimated, including demographic variables such as socioeconomic status, age, and sex. Socioeconomic status is especially important for PRSs of behavioural and neurocognitive traits of interest to psychiatry; alleles increasing risk for psychiatric disorders tend to be also associated with low socioeconomic status. Another issue that particularly affects PRSs for psychiatric, behavioural, and cognitive traits is genetic nurture: the fact that the genes of parents also shape the environment in which the offspring grow up, as a function of the expression of the parental genotype. Relative to conventional GWASs, within-family GWASs that control for genetic nurture (and population stratification due to ancestry effects) show considerably reduced estimates of R2 for PRSs of traits such as educational attainment, smoking, and depressive symptoms. By contrast, R2 for PRSs of non-psychiatric traits (such as height or diabetes risk) are not substantially diminished by within-family GWASs. Collectively, these findings highlight that psychiatric and behavioural traits are influenced by a complex interplay of genetics and environment, and additive SNP effects captured by PRSs represent only a fraction of these risk factors.”
As Lencz et al. (2022) note, PRS based on large population samples such as the UK Biobank are confounded by the effects of genetic nurture (genes of parents also shape the environment in which the offspring grow up). Within-family (or within-sibship) GWAS that attempt to control for that show substantially reduced estimates for cognitive and behavioral phenotypes that have been studied using this method. As far as I know, within-family or within-sibship GWAS for schizophrenia have not yet been conducted, and polygenic embryo selection is by its nature a scenario where within-family estimates are more relevant than population estimates.
Future environmental differences will modify the predictive accuracy of PRS in unknown ways.
Polyakov et al. (2022) write:
“It is important to note that PRS are derived from studies of people who have lived long lives in certain environments. It is also undoubtedly true that humans conceived today will live their lives in a radically different environment compared to people who were born 50 years ago. In the past 100 years, environmental conditions and lifestyle have changed dramatically, and these changes have accelerated in recent decades. The gene–environment interactions that produced a disease phenotype in people in their 50s and 60s are unlikely to be similar to the gene–environment interplay over the next 50 years. Thus, not only is it difficult to assess the clinical validity of PRS-ES in terms of the outcomes in question, it is also possible that clinical validity would be limited by the different effects of future environment on gene expression, compared to the past. This represents one of the inherent limitations of PRS, where the original study population may have been under different environmental influences compared to the populations to which PRS is applied.”
Relative risk reductions decrease (and absolute risk reductions increase) as the genetic risk increases.
The following estimates in figures are from Orchid’s risk calculator. We can see that as the family history of schizophrenia increases, there is correspondingly less and less risk reduction, such that in a scenario with both parents having schizophrenia, the relative risk reduction is 18% (absolute: 39% vs. 32%). In the scenario where one parent has schizophrenia, the estimated reduction in risk is 8.1% vs 5.6%.
