
Psychiatric Diagnosis: A Reintroduction
A guide for educators, trainees, clinicians, and critics

Psychiatric diagnosis remains mired in perpetual controversy, yet so much of the critique is directed at cliches and stereotypes of diagnosis (stereotypes that are unfortunately also promoted and reinforced by our currently impoverished state of mental healthcare) rather than our best conceptual understanding of it. In an effort to make such understanding more accessible to a wider audience, I present an introductory overview, making frequent use of quotes from relevant literature.
I organize my discussion along the following aspects:
Diagnosis-as-denotation and diagnosis-as-process
Recognizing a “syndrome”
The nature of diagnostic problem
Disorder attribution
Demarcating a syndrome from other syndromes (nosology)
Clinical significance
Symptom distribution and latent structure (categories vs dimensions)
Operationalized, indexical criteria
Modes of thinking/perspectives (nomothetic/idiographic, etc.)
Diagnostic pluralism
Diagnosis and context
1) Diagnosis-as-denotation and diagnosis-as-process
“We needn’t look far to recognize that diagnosis is used as both a noun (a denotation) and a verb (an action-bound process or procedure) in everyday clinical discourse... diagnosis as denotation implies categories and classification (names for things), and therefore poses one logical and pragmatic context for considering the diagnosis concept. However, considering the ‘approach’ to diagnosis — the process or procedure — we then look to the practices of clinicians working in particular contexts with particular people. Here the denotation ‘diagnosis’ (as with a DSM or ICD category) is only a portion of the story, perhaps even a modest portion.” John Sadler, Values and Psychiatric Diagnosis, p 417
Sadler makes a distinction between diagnosis-as-denotation and diagnosis-as-process. Where the former suggests categories and classifications, the latter points towards a broader notion of diagnostic practice. The two are interlinked. A categorization of psychopathology means little without some process of recognizing, understanding, and contextualizing psychopathology. Diagnosis is both the process and the outcome of ascertaining the nature of a clinical problem, it is an answer to the question “what’s going on here?”
Diagnosis is both the process and the outcome of ascertaining the nature of a clinical problem, it is an answer to the question “what’s going on here?”
The broader understanding of diagnosis immediately highlights the limitations of DSM and ICD: “The DSM’s strength is in its comprehensive catalogue of mental ills… but its weak spot as a textbook of psychopathology is its feeble handling of good, skillful, conscientious diagnostic practice. The DSM can help the clinician figure out the patient’s disorder, but it provides only a piece of the puzzle in figuring out ‘what’s going on here,’ and even less about how to figure out ‘what’s going on here.’” (Sadler, Values and Psychiatric Diagnosis)
2) Recognizing a “syndrome”
Descriptive diagnoses refer to an identifiable pattern of problems reported by the individuals and features observed by the clinician (symptoms and signs). When characterizing a cluster of symptoms as a syndrome, there is an assumption that the pattern is not random or a chance co-occurrence, and that the co-occurrence and co-variation is legitimate. This by itself is not a causal explanation but it is the beginning of one: it points towards the need for something to be explained. It is not merely a convenient shorthand for a list of symptoms, because we are assuming there is a relationship between the symptoms. There has been a tendency to assume that the pattern exists because of a “common cause” or a “latent variable” which produces the symptoms, but the scientific community is much more aware now that explanations can take other forms (e.g., symptom networks in which symptoms reinforce each other to create a self-sustained feedback loop in the absence of a central mechanism).
We can think of syndrome identification and recognition as:
a recognition of individual symptoms
a recognition that symptoms form a pattern
looking for statistical evidence of co-occurrence and co-variation
attempts to validate the pattern by looking for evidence (is the pattern associated with differences in risk factors, course, prognosis, treatment response etc.)
an assumption that there are mechanisms responsible for co-occurrence
hypotheses about what those mechanisms are
It is often said that descriptive psychiatric diagnoses don’t explain anything… This is not quite true. The criticism conflates etiological or causal explanation with other forms of explanation. One such form of explanation might be described as pattern recognition and matching (“formal cause,” if you prefer thinking in Aristotelian terms). “Your presentation matches this well-recognized pattern of symptoms, and not these other patterns, and we can use this pattern to link your presentation with existing knowledge from clinical experience as well as research that has been conducted on this pattern and treatments that have been investigated for this pattern.” This may not be an etiological explanation, but it is not simply a tautological repacking of symptoms.
Symptom patterns are connected with other information of interest to us – these are known as validators, and include things like genetics, family history, risk factors, course of illness, treatment response, etc.
The common idea that diagnosis offers no more information that the patient’s presenting complaints is also not true. This fails to appreciate that diagnosis is the end product of a diagnostic evaluation. A diagnostic evaluation is a careful consideration of the various possibilities relevant to a person’s complaints. A patient may present with depressed mood but the psychiatrist may arrive at a diagnosis of “Obsessive Compulsive Disorder” or “Alcohol Use Disorder” based on a careful history and evaluation, even when the patient may not have been thinking in those terms. A patient may present with anxiety, and get a diagnosis of a psychotic disorder. If we don’t take into account the process of diagnostic evaluation, we fundamentally fail to grasp what a diagnosis is and what it does.
3) The nature of diagnostic problems
Medical diagnoses are an eclectic mix of symptoms, syndromes, injuries, syndromes with well-defined etiologies, and diagnoses in terms of pathological change. Physicians use diagnoses like “chronic low back pain,” “dyspepsia,” “tension headache,” “urinary retention,” as much as they use diagnoses like “glioblastoma multiforme.”
Ahmed Samei Huda (The Medical Model in Mental Health, p. 38) notes that a variety of problems and conditions may be classified with a diagnosis:
“A broad category of clinical problems for which a specific condition has not been identified yet, such as ‘acute abdominal pain’, or of persisting clinical problems despite an identified diagnosis.
A classic disease or syndrome clearly demarcated from good health and each other in the form of syndromes.
A spectrum between health and illness with an unclear demarcation, or boundary, set between the two;
A spectrum of illness or condition with an unclear demarcation set between these illnesses or conditions.
Spectrums of illnesses or conditions with frequent co-occurrence.
Injuries.
Other conditions that are felt to be of interest to healthcare professionals but that are not illnesses, such as pregnancy.”
4) Disorder attribution
A common practice in contemporary psychiatry – exemplified by the DSM – is the tendency to refer to most diagnostic problems/syndromes/constructs as “disorders.” For example, Generalized Anxiety Disorder consists of the “Generalized Anxiety” syndromic construct and the characterization of this syndrome as a disorder.
There is an extensive literature on the concept of “disorder” (and related concepts such as disease, dysfunction, and illness), which is difficult to summarize here. There is no philosophical consensus on how “disorder” should be defined or understood. There are many approaches available to us. Many commentators have even challenged the need for such a unitary concept.
We may think of one strand of disorder concepts as focusing on the clinical context, centered on practical considerations of harm (distress, disability, impairment, disruption, etc.) and practical judgments that something has gone wrong, that the individual is experiencing a state that is out of the ordinary, that violates our usual expectations of what is typical, rational, meaningful, proportional, or understandable within a context.
The other strand focuses on biological and natural functions… functioning as it is described by an account of natural functioning. For example, Christopher Boorse thinks of health in terms of normal species functioning, i.e. the statistically typical contribution of all the organism's parts and processes to the organism's overall goals of survival and reproduction. Jerome Wakefield thinks of function in terms of a trait performing its evolved function (for which it has been naturally selected). There are other notions as well. Disease/dysfunction then is a departure from or failure of natural function.
The important thing amidst such discord is to have clarity on what notion of “disorder” is being utilized, if one is using that term. A common misconception is that “disorder” refers to a biological disease entity. This misconception is reinforced by clinicians who describe mental illnesses as “chemical imbalances” or “diseases just like diabetes.”
Some clinicians understand disorder almost entirely in terms of distress, impairment, and harm, and they may use it as a synonym for a problem that warrants clinical attention, but usually there are folk judgments of abnormality implicit in such judgments.
DSM-5 defines mental disorder as a syndrome characterized by clinically significant disturbance in an individual’s cognition, emotion regulation, or behavior; this disturbance reflects a dysfunction in the psychological, biological, or developmental processes underlying mental functioning. DSM-5 further states that mental disorders are usually associated with significant distress or disability, the latter evident in social interaction, and in occupational or other activities.
Here’s how Ken Kendler describes the DSM notion of dysfunction:
“The general idea of dysfunction is common-sensical – that the relevant psychobiological system is not doing what it is supposed to do. Examples might include providing your higher centers with an approximately veridical sense of the world around you, keeping levels of anxiety roughly appropriate to the real dangers being confronted, producing mood states approximately congruent to the environmental situation, etc. DSMs have traditionally seen disorders as existing within individuals and, for example, avoided providing diagnoses for dysfunctional marriages or families. So, in that sense, the underlying disturbance is seen to exist within individuals. I do not see that definition having much of anything to do with the causes. Environmental experiences like severe childhood sexual abuse can clearly cause dysfunctional mood-modulation systems as well as a high genetic vulnerability.”
With a broad notion of “disorder” relying on common-sensical, practical, and folk judgements, most clinical conditions and problems are characterized as “disorders” and with a narrower notion relying on natural function/dysfunction, some undetermined subset of clinical problems would be appropriately described as “disorders.” At present, diagnostic manual and clinical practice utilize a broad notion of “disorder.” Given that “disorder” does come with implicit or explicit assumptions of dysfunction, some prefer using more neutral terms such as clinical/ medical/ psychological “condition” or “problem.”
See also:
Aftab A, Rashed MA. Mental disorder and social deviance. International Review of Psychiatry. 2021;33(5):478-85. [access pdf here]
Kukla QR. What Counts as a Disease, and Why Does It Matter?. The Journal of Philosophy of Disability. 2022.
5) Demarcating a syndrome from other syndromes (nosology)
When causal and etiological mechanisms are well-understood, medicine and psychology are able to use them to categorize conditions, but even when etiology is known, if the mechanisms are too complex or dimensional, we have to rely on pragmatic considerations to draw boundaries and set thresholds.
From a somewhat simplified metaphysical perspective, we may think of a classification as demarcating natural kinds, practical kinds, or social kinds. If psychiatric classification were classifying natural kinds, we’d expect each diagnosis to correspond to an entity that exists in structure of the world independent of human interests. That is clearly not the case. If psychiatric classification were classifying social kinds, we’d expect them to be almost entirely socially constructed – like political borders between countries. Or recall Borges classifying animals into categories such as “those belonging to the Emperor” and “trained ones” in a fictional ancient Chinese encyclopedia. This may be considered a skeptical view of psychiatric classification endorsed by some critics.
From a somewhat simplified metaphysical perspective, we may think of a classification as demarcating natural kinds, practical kinds, or social kinds.
By and large, however, psychiatric kinds, as we currently understand them, appear to be practical kinds. Practical kinds are useful heuristic constructs that “carve up” the neurophysiological and psychological space in ways that serve our clinical and scientific goals. This view is best articulated by Peter Zachar.
Zachar: “Kinds can be demarcated on the basis of causal processes, but it is a simplification to say that causal processes uniquely fix which demarcations are relevant for different practical purposes. The world has many “joints,” but carving occurs with respect to goals and purposes. To push the metaphor a bit: How we carve a chicken will depend on whether we are making chicken soup, fried chicken, or curry chicken with white meat. White meat is an objective property in the world, but to "find it" we have to slice through some bones. It is present in the world independent of our interests, but it is not demarcated by the world alone. The same is true of kinds of psychiatric disorders.” [Zachar, P. (2014). Beyond natural Kinds: Toward a ‘Relevant’ ‘Scientific’ Taxonomy in Psychiatry. In: Classifying psychopathology: Mental kinds and natural kinds, 75-104.]
Zachar: “I am skeptical of a privileged, correct psychiatric classification as well, but the ways in which symptoms empirically cluster together likely places constraints on psychiatric classification that don’t apply to organizing libraries. If we could encounter a psychiatric classification manual from a parallel historical trajectory, I suspect we would recognize something of ours in the classifications of those who lived the alternative history even if they carve things up quite differently.” (2020)
Here is Huda in The Medical Model in Mental Health (p 49-50):
“The purpose of classification in clinical practice is clinical usefulness. If it is impossible to delineate clearly separate categories, either because they do not exist because the condition is a spectrum or because we lack the capability to demonstrate the boundaries between conditions, then the next best option is to use a clinically useful classification based on identifying points on a spectrum. As long as people are aware that they aren’t necessarily describing clearly separate categories—either from states considered healthy or from other conditions—then, if a diagnosis can be reliably distinguished from other diagnoses and carries clinically useful discriminatory information (such as likely range of outcomes or different responses to treatment), it is a ‘worthwhile’ diagnosis.”
For a more detailed conceptual and historical discussion of psychiatric classification, see Aftab A, Ryznar E. Conceptual and historical evolution of psychiatric nosology. International Review of Psychiatry. 2021;33(5):486-99. [access pdf here]
6) Clinical significance
Clinical diagnosis is not about knowledge for the sake of knowledge. Clinicians are interested in identifying and classifying matters of practical concern. The underlying idea behind “clinical significance” is that the nature or severity of the problem is such that it leads to the individual (or their social circle) seeking the help of a professional or such that the condition comes to clinical attention via its disruptive or harmful effects on self or others.
Appreciating clinical significance therefore opens us up to the wider appreciation that diagnostic manuals are “actually compilations of the sorts of things that physicians treat; a circular classificatory principle but a useful historical clue. Our definitions of illness are derived from medical practice.” (Donald Klein) This also raises questions about the social organization that results in these kinds of problems being brought to psychiatric attention as opposed to elsewhere, and is relevant to the disorder vs deviance debate.
7) Symptom distribution and latent structure (categories vs dimensions)
Diagnosis may be described in categorical or dimensional terms. This is a broad and complex topic requiring a detailed discussion, so I will restrict myself to a brief quote and some references
“One of the challenges of any scientific discipline is to determine which of its variables are categorical (i.e., qualitative differences exist between groups of people or objects) and which of its variables are dimensional (i.e., people or objects differ quantitatively along one or more continua). Although a variable may be conceptualized and measured categorically or dimensionally, this need not correspond to its true latent structure. For example, clinical interviews that are used to diagnose mental disorders according to published criteria yield categorical data reflecting the presence or absence of each disorder. In contrast, many self-report or clinician-rated scales yield dimensional data representing the severity of symptoms or disorders. In either case, the dichotomous or dimensional nature of the data may be an artifact of the measurement approach, masking the underlying reality. Fortunately, methodological tools are available to evaluate empirically whether a variable is categorical or dimensional at a latent level, regardless of how it has been conceptualized or measured.” (Ruscio & Ruscio, 2008)
For an example of a dimensional classification of psychopathology, see HiTOP.
See also: Haslam N, McGrath MJ, Viechtbauer W, Kuppens P. Dimensions over categories: A meta-analysis of taxometric research. Psychological Medicine. 2020;50(9):1418-32.
8) Operationalized, indexical criteria
The official criteria used in diagnostic manuals such as DSM are a (fallible) way of identifying or indexing a syndrome or clinical condition. These criteria are not constitutive; it is not the case that having a disorder is nothing more than meeting the diagnostic criteria.
“We all know that the current DSM diagnostic criteria have been selected because they usefully index our disorders. Many other symptoms and signs could have been used, but the ones selected, often by clinical tradition rather than careful scientific selection, have been shown to perform well. However, in many ways, we act as if the DSM criteria constitute our disorders. We teach our residents to focus their evaluations largely or solely on assessment of DSM criteria. Our clinical and research structured interviews assess only DSM criteria. Our treatment algorithms utilize DSM categories evaluated by DSM criteria. Our large epidemiological surveys typically assess only the diagnostic criteria for each DSM category. We act as if the DSM criteria are all that really matter when it comes to evaluating psychiatric illness.
In our teaching, we should consistently remind trainees that DSM criteria are a good place to start for a diagnostic evaluation, but that examining only these symptoms and signs would lead to an impoverished view of psychopathology. In our clinical work, we should remember to explore the diversity of the pathological experiences of our patients, with the DSM criteria being only a good jumping off point for further inquiry. For our research, we should insist on sampling beyond the DSM criteria to capture more of the wide domains of symptomatology for the disorders we are examining. After all, how can we possibly improve on our current criteria if our large data sets are restricted to these limited sets of signs and symptoms?”
9) Modes of thinking/perspectives
“Nomothetic and idiographic are terms originally used by philosopher Wilhelm Windelband to describe two distinct approaches to knowledge. Nomothetic describes a tendency to describe phenomena in terms of general laws and scientific categories, while idiographic describes a tendency to understand unique and specific phenomena. In psychology and psychiatry, the idiographic approach emphasizes the subjectivity and psychological history of the individual.” (Aftab & Ryznar, 2021)
The characterization of the problem in a diagnostic context may come in nomothetic or idiographic forms. The emphasis has been on nomothetic in formal nosologies but diagnosis, in the broad sense, requires some combination of both. This is because clinical problems encountered by patients have some attributes shared by others but also some attributes that are unique to them. Even heavily idiographic approaches nonetheless must rely on some sort of nomothetic schema, otherwise there would be no way to compare one individual’s clinical problem to another.
Even heavily idiographic approaches nonetheless must rely on some sort of nomothetic schema, otherwise there would be no way to compare one individual’s clinical problem to another.
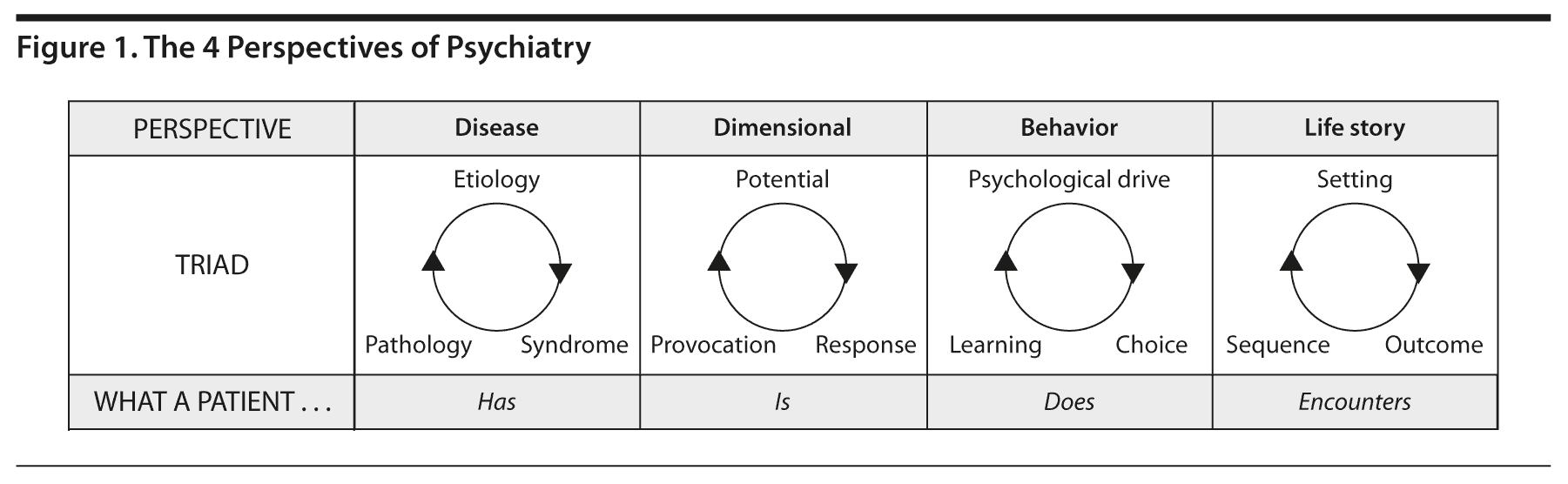
See also: McHugh and Slavney’s four perspectives of disease, dimensions, behavior, and life story to clinically understand psychiatric problems (figure below taken from the article).
10) Diagnostic pluralism
John Sadler: “As McHugh and Slavney have argued before me, clinical phenomena support a profound range of ways to describe them, understand them, explain them, and intervene with them. Such a pluralism of perspectives means that to limit our clinical viewpoints to just one or two will impoverish our understanding of the whole.” “… it seems to me likely that a clinical classification of mental disorders has much to offer clinical (patient-oriented) and systems (healthcare delivery) research, but correspondingly little to offer basic neuroscience, genetics, cognitive psychology, and even the social science mental-health research endeavor. These latter disciplines will need their own categories, systems, and nomenclature to impose orders on daunting complexities.” (Values and Psychiatric Diagnosis, p 434)
Ahmed Samei Huda: “Given the element of subjectivity and the role of professionals in deciding which conditions constitute illnesses or diseases, is it the case that conditions labelled as illnesses or diseases should only be viewed with the medical model? Emphatically, no! … The medical model can thus be viewed as follows:
One way of conceptualizing and helping a condition and not necessarily the only way.
Not automatically the best way of helping to achieve all or indeed any desired outcomes.
A model that is willing work in conjunction with other models, in a multi-model, multidisciplinary way (i.e. with others such as carers, other professionals), each contributing a part to achieve desired outcomes.
A model that at times may be unhelpful or even harmful for certain conditions.”
(The Medical Model in Mental Health, p. 14)
11) Diagnosis and context
Sadler: “… many of the controversies associated with psychiatric diagnosis and the DSMs have to do with an incomplete appreciation of the dual meaning of diagnosis: as denotation and as practice… [Critics] construct a straw clinician when they suggest that DSM-style diagnosis is decontextualized… The DSM diagnosis is decontextualized until it is applied by a clinician with diagnostic finesse. The DSM is decontextualized and decontextualizing only if it is split away from the context of good clinical practice… The problem is more that the DSM just doesn’t spell out enough what good practice is. Diagnostic virtue is more-or-less lost in the catalogue’s instructions.” (Values and Psychiatric Diagnosis, p 429-431)
This is by no means a comprehensive or exhaustive discussion, there is a lot more to say and discuss. My positive assessment of John Sadler’s Values and Psychiatric Diagnosis and Ahmed Samei Huda’s The Medical Model in Mental Health must be obvious from my use of heavy quotations from these works. Readers are encouraged to consult them for their comprehensive treatments of the subject, and I will have more to say about psychiatric diagnosis on this newsletter later as well.
Relevant posts from Psychiatry at the Margins: