
The Boundaries of Palliative Psychopharmacology
Article in AMA Journal of Ethics

My latest peer-reviewed article, “What Should Clinicians Know About Palliative Psychopharmacology?” in the AMA Journal of Ethics examines conceptual uncertainties around palliative use of psychopharmacology, and offers an account of palliative psychopharmacology by focusing on modifiable and unmodifiable aspects of a condition. The article is open-access, and you are welcome to check it out. I’ll post some excerpts below.
“This demarcation problem brings uncertainty to the practice of palliative psychopharmacology, with attendant ethical consequences. If we present palliative treatment as curative, we generate an erroneous idea that the etiological causes or the causal mechanisms of the distressing and impairing states are being addressed. By the same token, adopting a palliative approach prematurely or inconsistently—for instance, by opting for symptomatic pharmacological relief without addressing modifiable psychosocial factors that causally contribute to the persistence and severity of the psychiatric illness or by failing to recognize that one has shifted from a curative to a palliative approach—is ethically significant, since doing so may result in an inadvertent narrowing of the focus of clinical care, with suboptimal outcomes. How, then, to conceptualize the relationship between psychiatry and palliative care?”
“We can extract 2 sorts of views about palliative psychopharmacology [in the existing literature]: one view, exemplified by Trachsel et al and Balon et al, focuses on whether medications are symptom reducing or disease modifying and, to the extent that psychiatric medications are symptom reducing, maintains that they are potentially palliative (provided they are used in the appropriate clinical context). According to the other view, exemplified by Westermair et al, medications are curative if used with the goal of symptom reduction and palliative if the goal is not symptom reduction but improved quality of life. As I will explain, both approaches encounter significant limitations.”
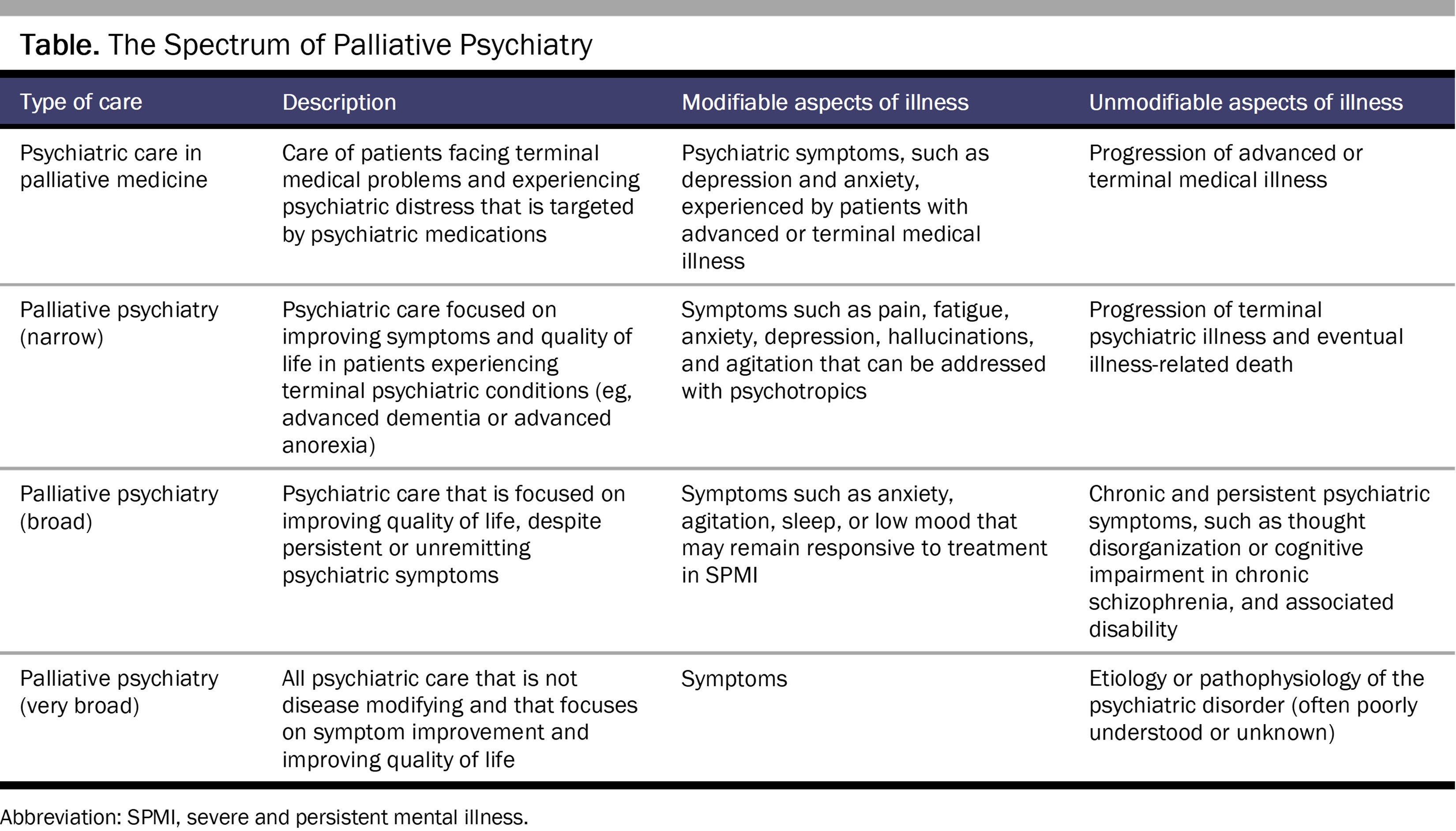
“In my view, the relevant distinction in palliative psychopharmacology is not etiology vs symptoms or symptoms vs quality of life, but rather modifiable vs unmodifiable aspects of illness in relation to quality of life—aspects that may be either etiological mechanisms or symptoms. My use of the term unmodifiable is also intended to describe situations in which we have decided not to modify an aspect of the illness in the interest of prioritizing quality of life. The essence of palliative care, I suggest, is when we are forced to work around an aspect of the illness to enhance quality of life. This aspect will be different in different situations.”
The essence of palliative care, I suggest, is when we are forced to work around an aspect of the illness to enhance quality of life. This aspect will be different in different situations.
“We can make further fine-grain distinctions as well. For instance, the severity of symptoms may be modifiable but not their persistence (for instance, hallucinations may become less intense or less frequent but otherwise continue to be experienced); acute episodes may be modifiable but not their recurrence (for instance, for some patients, antidepressant medications may alleviate an active episode of depression but may not successfully prevent future episodes). These examples serve to illuminate the dimensionality of palliative goals and their overlap with curative goals. What distinguishes any particular instance of care as palliative is an emphasis on quality of life and an acceptance of the unmodifiable aspects of an illness.”
“Consider the use of intravenous ketamine (or intranasal esketamine) to treat severe and persistent depression that has proven refractory to standard treatments. If the goal is remission or significant alleviation of depressive symptoms, this intervention will not typically qualify as palliative. However, consider other possible outcomes of treatment: ketamine temporary relieves depression but the depression inevitably returns (unmodified recurrent course); ketamine reduces depression severity but the depression persists otherwise (unmodified chronicity and persistence); or the depression is unaltered but the psychoactive experiences (eg, euphoria, dissociation) make depression more tolerable for the patient (unmodified symptoms). If treatment is continued in the case of such outcomes, these goals can reasonably be considered palliative. Whether ketamine treatment increases or decreases quality of life and by what pathway can’t be determined in advance for a particular individual. Similar considerations can also apply to other psychotropics, such as antidepressants for which it is possible that different individuals experience benefit via different pathways. A consequence of this view is that clinicians have an ethical imperative to distinguish among and clearly formulate goals of care in a dynamic and ongoing process of shared decision making with patients.”
Kudos for your very thoughtful paper, Awais! I agree with the statement in your paper:
"...uncertainty about the evidence complicates labeling an intervention as disease modifying or symptom reducing. In particular, if we link the palliative status of psychopharmacological treatment to whether or not it is disease modifying, we’d have to acknowledge that there is a lack of scientific consensus on the matter, precluding us from saying with certainty whether the intervention is palliative or not."
Indeed, I believe that a binary approach to these terms is not helpful. A pharmacological intervention may be both disease modifying and symptom reducing, in varying proportions; and a putative binary distinction would require a complete--or nearly complete--understanding of both the disease process and the precise mechanism of action of the medication.
In my view, we do not have that degree of understanding for the major psychiatric diseases, or for the medications we use to treat them. I believe this limitation applies to the use of antipsychotic, antidepressant, and most mood stabilizing medications.
I prefer the term "life-modifying" to either "disease-modifyng" or "symptom reducing". "Life-modifying" implicitly invokes the critical--and under-emphasized--concept of "quality of life", which you rightly highlight. A medication that substantially improves the patient's quality of life--defined using scales such as the QOLS [1]--may be considered a "life-modifying" medication.
This construct does not commit us to answering the question of whether the medication alters the underlying disease process (to the extent we even know what this is) or whether it "merely" relieves symptoms. (I think symptom relief has been vastly under-rated as a central goal in psychiatry).
Of course, understanding and modifying the underlying disease process (or, more likely, processes) is devoutly to be wished, but may simply be beyond our reach, for most psychiatric diseases--at least, in our present state of knowledge.This acknowledgment should not lead us to disparage our treatments, and the positive difference they can make in a patient's life. (Yes, there are side effects and risks, as well--as with literally every somatic treatment in the field of medicine). This point was recently made in a study of antidepressants and "quality of life". [2] The study concluded--rightly, in my view--that "patients with depression benefit more from treatment than is suggested by only examining outcome from a symptom-based perspective."
Kind regards,
Ron
Ronald W. Pies, MD
1. https://pubmed.ncbi.nlm.nih.gov/14613562/
2. https://www.medscape.com/viewarticle/995195?ecd=mkm_ret_230902_mscpmrk_psych_anxiety_etid5811850&uac=430527SG&impID=5811850#vp_2