
Assisted Outpatient Treatment: A Summary of the Evidence
No study has demonstrated that involuntary outpatient treatment adds value beyond the enhanced services and system accountability that accompany it.

Nev Jones, PhD, is an Associate Professor of Social Work and affiliate faculty in the Department of Psychiatry at the University of Pittsburgh, USA. An accomplished mental health services researcher, her work has been continuously funded by the National Institutes of Health and she leads multiple large-scale research projects focused on systems and services for individuals labelled with ‘serious mental illness.’ Along with colleagues from the Human Services Research Institute, she recently completed a large-scale study of the implementation and effectiveness of AOT across New York State.
What Is Assisted Outpatient Treatment?
Assisted Outpatient Treatment (AOT), also known as Involuntary Outpatient Commitment (IOC), is a civil court procedure in which a judge orders an adult with a serious mental illness to adhere to community-based treatment. In the United States, as of 2024, 48 states and the District of Columbia authorize some form of AOT. Implementation varies widely across and within states in eligibility criteria, duration of court orders, available services, and enforcement mechanisms.
AOT typically involves mandated medication (often long-acting injectables), required attendance at outpatient appointments, substance use restrictions, and case management monitoring. Noncompliance may result in law enforcement transport to a hospital for evaluation, and potentially involuntary hospitalization or medication over objection. Court orders are typically 90–180 days, renewable indefinitely in most states.
What Do the Randomized Controlled Trials Show?
Three randomized controlled trials (RCTs) of involuntary outpatient commitment have been conducted worldwide. RCTs are the gold standard for determining whether an intervention causes better outcomes, because random assignment controls for all other factors that might explain differences between groups.
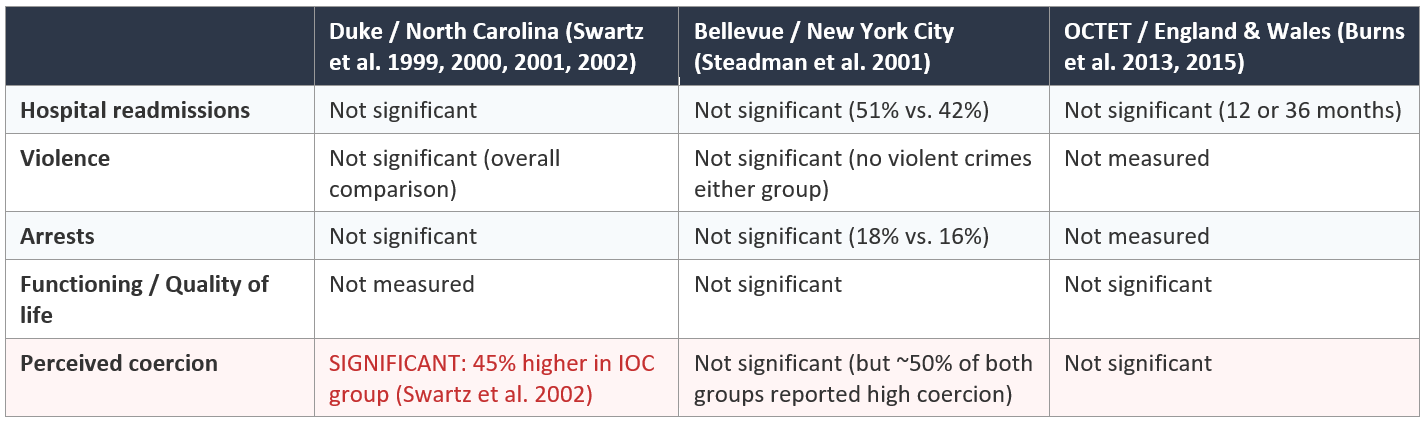
Key findings: None of the three RCTs found statistically significant differences between court-ordered and control groups on any primary clinical outcome. The Duke study reported positive results only in secondary, post-hoc subgroup analyses — specifically, for individuals whose court orders were sustained for 6+ months and who also received intensive services (3+ contacts/month). However, commitment duration was not randomly assigned, and the Cochrane Collaboration, which sets international standards for evidence-based review, treats post-hoc subgroup findings that contradict null primary analyses as having low evidentiary value.
The most recent (‘Gold Standard’) Cochrane meta-analysis (Kisely & Campbell, 2017), pooling all three RCTs, found no significant effect of court-ordered treatment on any of the meta-analyzable clinical outcomes studied with the exception of low quality evidence for reduced victimization. The number needed to treat (NNT) to prevent one hospital readmission was calculated as 142 — meaning 142 individuals would need to be placed under court orders to prevent a single hospitalization. While AOT is typically justified as a means of addressing “violence” or “social harm” in the US, recent meta-analysis of all available research on the effects of involuntary outpatient treatment on aggression or criminal offending found no significant benefits in either primary or sub-group analyses (Kisely et al., 2025).
Notably, in the Duke study, besides reduced victimization, coercion was the only other variable that reached statistical significance in a primary between-group comparisons: individuals under court orders reported 45% higher coercion than controls who received the same services without a court order. Black participants were approximately twice as likely to experience high levels of coercion as white participants, and disproportionality remained even after controlling for diagnosis, symptom severity, substance abuse, insight, functioning, marital status, and the length of the court order (Swartz et al. 2002).
What About Non-Experimental Studies?
Since the Duke and Bellevue RCTs, no further randomized trials of AOT have been conducted in the United States. The post-2001 evidence base consists of pre-post (mirror-image) studies, quasi-experimental matched comparison research, and the 2024 federal ASPE evaluation. These studies generally report improvements in hospitalizations and service utilization after AOT enrollment. However, they share fundamental limitations:
• Regression to the mean. Individuals are enrolled in AOT at their worst point — after repeated hospitalizations or crises. Statistical improvement from that low point is expected regardless of intervention. Only comparison to a control group can account for this, and non-experimental studies lack true control groups. Studies of voluntary ACT as well as studies comparing ACT and AOT (as is true of the ASPE evaluation) find decreases in all areas for individuals receiving voluntary ACT, not just AOT.
• Confounding of court orders with enhanced services. AOT enrollment typically comes with priority access to assertive community treatment (ACT) or intensive case management, linkage to SSI/SSDI and other social welfare benefits and sometimes guaranteed access to supportive housing. When hospitalizations or arrests decrease after someone begins receiving ACT and/or supported housing, attributing that improvement to the court order rather than the services is not justified.
• Provider accountability confound. AOT creates mandated accountability for providers to deliver services. This monitoring and accountability effect may itself drive improved service delivery, independent of the legal coercion experienced by the individual.
• Insufficient quantitative measurement of harm (see also below and cf Kisely et al., 2024 meta-analysis of what has and has not been documented to date globally).
The largest non-experimental study is the original New York State Kendra’s Law evaluation (Gilbert et al., 2010; Swartz et al. 2010), which analyzed Medicaid claims for 3,576 AOT recipients. The pre-post analyses showed reduced hospitalizations and increased service utilization. A contemporary New York-based quasi experimental study (Phelan et al. 2010) found some positive benefits, albeit with uncertain service utilization and provider accountability differences between AOT recipients and matched (quasi-experimental controls) but found no significant differences in psychotic symptoms or quality of life. The authors concluded that results “should be interpreted in terms of the overall impact of outpatient commitment, not of legal coercion per se.” Researchers at the University of Pittsburgh and Human Services Research Institute have recently completed a second, state-sponsored evaluation of Kendra’s Law – report will be released in early summer 2026.
ASPE Federal Evaluation and GAO Assessment
In 2024, the Office of the Assistant Secretary for Planning and Evaluation (ASPE) published a federally funded evaluation of SAMHSA’s AOT Grant Program, conducted by RTI International, Policy Research Associates (PRA), and Duke University School of Medicine. The evaluation examined 6 case study sites selected from 18 federally funded programs and used within-group pre-post analyses supplemented by a between-group comparison at a single site. Most measures were collected through structured interviews with AOT recipients conducted by clinicians working at their sites, creating potentially far-reaching measurement bias as participants already under court orders and motivated to appear “compliant” and “happy” in order to discharge their orders would generally not be expected to honestly report concerns and negative outcomes directly to clinicians with (plausible) power over future decisions to renew.
In July 2025, the U.S. Government Accountability Office (GAO) reviewed the ASPE evaluation and SAMHSA’s outcome reports and concluded:
“HHS’s assessments of the effects of the AOT grant program were inconclusive. This is because the ASPE and SAMHSA assessment efforts were both hampered by methodological challenges, many of which were inherent in the program and beyond their control.”
The GAO declined to report the specific results of either the ASPE evaluation or SAMHSA’s reports to Congress, stating that they “decided not to include the evaluation’s results because (1) we determined that ASPE and RTI International lacked information needed to help understand the extent to which the results represented all AOT participants included in SAMHSA’s grant program; and (2) our analysis of information we received from RTI International showed a high level of uncertainty for some of the results.”
Since 2016, the federal government has awarded approximately $146 million in AOT grants to 63 grantees across 28 states. The GAO concluded that “challenges assessing the grant program are likely to persist.”
Coercion and Potential Harms
Although AOT’s defining feature is legal coercion, remarkably few studies have measured the experience or consequences of that coercion. The available evidence includes:
• The Duke North Carolina study (Swartz et al. 2002) found that court-ordered treatment increased perceived coercion by 45% compared to controls receiving the same services. Each additional month under a court order increased the risk of high perceived coercion by approximately 10%. African American race independently predicted nearly twice the odds of experiencing high coercion (OR=1.89), after controlling for all measured clinical and demographic variables.
• Munetz et al. (2014) compared 17 former AOT participants to 35 mental health court graduates in Ohio. AOT recipients reported significantly higher perceived coercion on every dimension measured compared to mental health court participants, significantly lower procedural justice in interactions with judges, significantly less respect after program completion, and significantly less hope after completion than before.
• The judicial process itself raises substantial procedural justice concerns. A qualitative study of 13 NYC judges and 20 attorneys (Player 2015) found that judges overwhelmingly defer to the single evaluating psychiatrist, apply the evidence standard loosely, and rarely credit testimony from the individual subject to the order. Defense attorneys reported that their clients’ testimony often “means nothing” in practice and that psychiatric evaluations are typically 15–60 minutes conducted by clinicians with no prior treatment relationship.
Additional areas of potential harm that have not been published in the US AOT context include:
• Serious medication side effects from mandated polypharmacy, often without adequate access to treatment or intervention (beyond screening), including metabolic syndrome, Type II diabetes, antipsychotic-induced Parkinsonism, and cognitive decline secondary to the anticholinergic effects of prescribed medications.
• Custodial iatrogenesis: institutionalization in the community through supervised residential facilities that control finances, food, and social life creating dependency and de facto social and physical segregation.
• Disruption of family bonds including custody, elder caregiving and reproductive justice concerns – AOT orders may separate parents from children, and children from elderly parents, require residence in facilities that custodial parents have described as “too terrifying to expose a young child too” and/or that are physically distant; reproductive justice concerns include medication side effects impacting fertility, pregnancy and potential iatrogenic effects on the developing fetus.
• Social defeat — the chronic experience of subordination and powerlessness that is itself implicated in the development and worsening of psychosis.
These harms are non-trivial and publications in preparation (Pitt PathLab team) are beginning to document and substantiate how profoundly impactful they can be.
The Central Policy Question
The policy question underlying AOT is not “do people improve after AOT enrollment?” — pre-post studies can answer that question affirmatively for virtually any enhanced service, including voluntary ACT, supported housing, and SSI/SSDI access. The relevant question is: does the court order produce better outcomes than the same services delivered voluntarily?
The three randomized controlled trials that were designed to answer this question all found null primary results. The Cochrane meta-analysis confirmed no significant effect based on the pooling and re-analysis of data across RCTs. The most recent federal (ASPE) evaluation was deemed “inconclusive” by the US General Accountability Office upon audit and independent analysis of evaluation data. Meanwhile, the one participant-centered outcome measured in the Duke RCT — perceived coercion — is significantly increased by AOT, disproportionately for Black individuals, and the international qualitative research confirms widespread experiences and negative impacts of coercion within AOT (Barti et al., 2022; Goulet et al., 2020). No study has demonstrated that involuntary court-ordered treatment adds value beyond the enhanced services and system accountability that accompanies it. Meanwhile, intensive voluntary services such as ACT and Housing First have a well-established evidence base for improving outcomes for individuals with serious mental illness. Policymakers considering AOT should weigh whether the documented costs of legal coercion, in combination with serious ethical concerns, are justified given the absence of evidence that court orders add benefit beyond what these voluntary services achieve.
Join Nev Jones for an online webinar, A Deeper Dive on US “AOT” literature & International Findings, arranged by Roots Up, Mar 11 from 12pm to 2pm EDT.
Comments are open.
See also:



Key References
Bartl, G., Stuart, R., Ahmed, N., Saunders, K., Loizou, S., Brady, G., ... & Lloyd-Evans, B. (2024). A qualitative meta-synthesis of service users’ and carers’ experiences of assessment and involuntary hospital admissions under mental health legislations: a five-year update. BMC psychiatry, 24(1), 476.
Burns, T., Rugkåsa, J., Molodynski, A., Dawson, J., Yeeles, K., Vazquez-Montes, M., ... & Priebe, S. (2013). Community treatment orders for patients with psychosis (OCTET): a randomised controlled trial. The lancet, 381(9878), 1627-1633.
Burns, T., & Molodynski, A. (2014). Community treatment orders: background and implications of the OCTET trial. The Psychiatric Bulletin, 38(1), 3-5.
Burns, T., Yeeles, K., Koshiaris, C., Vazquez-Montes, M., Molodynski, A., Puntis, S., ... & Rugkåsa, J. (2015). Effect of increased compulsion on readmission to hospital or disengagement from community services for patients with psychosis: follow-up of a cohort from the OCTET trial. The Lancet Psychiatry, 2(10), 881-890.
Gilbert, A. R., Moser, L. L., Van Dorn, R. A., Swanson, J. W., Wilder, C. M., Robbins, P. C., ... & Swartz, M. S. (2010). Reductions in arrest under assisted outpatient treatment in New York. Psychiatric Services, 61(10), 996-999.
Goulet, M. H., Pariseau-Legault, P., Côté, C., Klein, A., & Crocker, A. G. (2020). Multiple stakeholders’ perspectives of involuntary treatment orders: a meta-synthesis of the qualitative evidence toward an exploratory model. International Journal of Forensic Mental Health, 19(1), 18-32.
Government Accountability Office. (2015). Serious mental illness: HHS assessment of assisted outpatient treatment have yielded inconclusive results. GAO-15-700.
Kisely, S. R., & Campbell, L. A. (2015). Compulsory community and involuntary outpatient treatment for people with severe mental disorders. Schizophrenia Bulletin, 41(3), 542-543.
Kisely, S., Zirnsak, T., Corderoy, A., Ryan, C. J., & Brophy, L. (2024). The benefits and harms of community treatment orders for people diagnosed with psychiatric illnesses: A rapid umbrella review of systematic reviews and meta-analyses. Australian & New Zealand Journal of Psychiatry, 58(7), 555-570.
Kisely, S., Bull, C., & Gill, N. (2025). A systematic review and meta-analysis of the effect of community treatment orders on aggression or criminal behaviour in people with a mental illness. Epidemiology and psychiatric sciences, 34, e12.
Munetz, M. R., Ritter, C., Teller, J. L., & Bonfine, N. (2014). Mental health court and assisted outpatient treatment: Perceived coercion, procedural justice, and program impact. Psychiatric Services, 65(3), 352-358.
Phelan, J. C., Sinkewicz, M., Castille, D. M., Huz, S., & Link, B. G. (2010). Effectiveness and outcomes of assisted outpatient treatment in New York State. Psychiatric Services, 61(2), 137-143.
Player, C. T. L. (2015). Outpatient commitment and procedural due process. International Journal of Law and Psychiatry, 38, 100-113.
Simon, J., Mayer, S., Łaszewska, A., Rugkåsa, J., Yeeles, K., Burns, T., & Gray, A. (2021). Cost and quality-of-life impacts of community treatment orders (CTOs) for patients with psychosis: economic evaluation of the OCTET trial. Social psychiatry and psychiatric epidemiology, 56(1), 85-95.
Steadman, H. J., Gounis, K., Dennis, D., Hopper, K., Roche, B., Swartz, M., & Robbins, P. C. (2001). Assessing the New York City involuntary outpatient commitment pilot program. Psychiatric Services, 52(3), 330-336.
Swartz, M. S., Swanson, J. W., Wagner, H. R., Burns, B. J., Hiday, V. A., & Borum, R. (1999). Can involuntary outpatient commitment reduce hospital recidivism?: findings from a randomized trial with severely mentally ill individuals. American Journal of Psychiatry, 156(12), 1968-1975.
Swartz, M. S., Swanson, J. W., Hiday, V. A., Wagner, H. R., Burns, B. J., & Borum, R. (2001). A randomized controlled trial of outpatient commitment in North Carolina. Psychiatric Services, 52(3), 325-329.
Swartz, M. S., Wagner, H. R., Swanson, J. W., Hiday, V. A., & Burns, B. J. (2002). The perceived coerciveness of involuntary outpatient commitment: findings from an experimental study. Journal of the American Academy of Psychiatry and the Law Online, 30(2), 207-217.
Swartz, M. S., Wilder, C. M., Swanson, J. W., Van Dorn, R. A., Robbins, P. C., Steadman, H. J., ... & Monahan, J. (2010). Assessing outcomes for consumers in New York’s assisted outpatient treatment program. Psychiatric Services, 61(10), 976-981.
Valasek, C. J., Nelson, K. L., Fettes, D. L., & Sommerfeld, D. H. (2025). Emerging trends in research on assisted outpatient treatment in the United States: a narrative review. Psychiatric Services, 76(5), 469-478.
 | A guest post by
|
I’ve had odd and contradictory experiences with AOT.
Lots of patients being brought to the ED by AOT for supposedly not taking meds. Patients clearly not decompensated. Calmly sitting and saying that they did. Shrug shoulders, discharged.
On the flip side, had a patient that was clearly decompensating, and their mom told me they weren’t taking meds. When I reached out, AOT said the patient said they were taking their meds so that there was nothing they can do. I explained: “the mom said she’s not taking her meds and with medical certainty I can tell you she is not taking her medications”. They said “well she said she’s taking them, so we can’t do anything”. Shrug shoulders, patient further decompensated and gets involuntary admitted a month later.
Really interesting. I'm struck by how high the demands are for things to be "evidence-based" when it comes to suggesting less coercive treatment of psychiatric patients. This is a stark example of how low that threshold for "evidence-based" is when it comes to taking away rights and implementing coercive methods. 3 RCTs! I try not to be too flippant about this as these are serious questions. But this is frustrating!