
People Are Stumbling From One Misguided Narrative About the Medical Model to Another

I don’t particularly like the term “medical model.” It takes something diverse and dynamic—the theory and practice of medicine—and turns it into something circumscribed, fixed, and static (often, but not always, for the purposes of critique). There is no single “model” that adequately applies to medicine, just as there is no single model that adequately applies to clinical psychology or to social work.
The American Psychological Association dictionary defines the medical model as “the concept that mental and emotional problems are analogous to biological problems—that is, they have detectable, specific, physiological causes (e.g., an abnormal gene or damaged cell) and are amenable to cure or improvement by specific treatment.”
I consider this definition to be highly inadequate, if not inaccurate. “Biological problems” gets us off on the wrong foot. It would be more accurate to say that the medical model considers mental and emotional problems to be analogous to problems encountered in general medicine. The second, and more serious, error here is that it immediately restricts the range of possible options to “detectable, specific, physiological causes,” when in reality, medicine deals with a very wide range of problems. Physical health problems are an eclectic mix of symptoms, syndromes, injuries, and pathologies. Physicians deal with problems like “chronic low back pain,” “dyspepsia,” “tension headache,” “urinary retention,” and “metabolic syndrome,” as well as problems like “seizure disorder,” “congestive heart failure,” “appendicitis,” “multiple sclerosis,” “scurvy,” and “measles.” Physiological changes are not always detectable. Changes are not always specific. Causes are often environmental or traumatic, and highly influenced by social factors, which is why public health interventions can be so effective. Physical health problems are often consequences of social problems like poverty, homelessness, lack of insurance, racism, and domestic violence. You have to work one night in the emergency room to appreciate that. Medicine has no difficulty tackling injuries, but for some reason, people in the mental health field have to talk about the psychological injuries in an isolated, fractured manner (“trauma model” being distinct from the “medical model”… does everything have to be its own model!), as if trauma doesn’t interact with other things like one’s developmental trajectory, personality traits, genetic vulnerabilities, neurophysiology, and the sociocultural context to produce its effects. If anything represents the “medical model” of psychopathology, the DSM does, but even the DSM doesn’t define mental disorders in terms of hypothesized biological dysfunctions — contra the APA definition. DSM-5 refers to “a dysfunction in the psychological, biological, or developmental processes underlying mental functioning.”
The academic confusion around “medical model” is what it is, but it has had a particularly deleterious effect on public understanding of mental health problems. A recent article by Rose Cartwright in the Guardian (April 13, 2024) seems to be a perfect illustration of some of the ways in which the public conversation around the “medical model” has gone awry.1
Cartwright’s story starts with her crippling experience of intrusive thoughts and images and her initial relief in the diagnosis of obsessive-compulsive disorder (OCD) that brought her “astonishing clarity and relief.” Her clinicians framed OCD as an “illness,” which she took to mean, “mental disorders are diseases of the brain with organic, biological root causes.” This way of thinking was reinforced by the psychotherapists she encountered, who spoke about “misfiring” of the amygdala and psychotherapy as “rewiring the brain.” She says she co-opted this language and started talking about mental illness in these terms, becoming a “poster girl” for OCD.
A turning point came years later when she interviewed neuroscientist Claire Gillan for a podcast, and Gillan said “OCD is not a biological reality” and that biological abnormalities identified in studies for OCD “are by no means exclusive to OCD.” This was a shock to Cartwright, and she writes,
“I didn’t know this. I thought my brain shared the same abnormalities as everyone else with OCD and that these were the root causes of our obsessions; that we had brains that were measurably different from the brains of people with, say, ADHD or anorexia. I thought this was the definition of “official” diagnosis. Gillan explained that, on the contrary, psychiatric diagnoses are not based on biomarkers, they are subjective constructs.”
What Cartwright is describing here is the classic essentialist view of psychiatric categories: that there is a particular feature (a brain abnormality in the biologically reductive view, but technically it could be any biological or psychological feature) shared by all people with a certain diagnosis that differentiates them from people with other diagnoses who do not possess that feature.
It is unlikely that this was explicitly communicated to Cartwright by any clinician. It is also unlikely that she read this in any psychiatry or psychology textbook. But essentialist assumptions about clinical and scientific phenomena are highly prevalent in the general population, and vague language such as “OCD is an illness, just like diabetes” can be enough to lead people to think that an essentialist view is being communicated to them.
Gregory L. Murphy writes in Categories We Live By:
“People believe in essences even if they have no idea what they are. It is a matter of faith that there must be some genes that make dogs dogs—genes that all of them share, even if one has no clue what those genes might be. Prior to modern biology, people also had that belief, though they didn’t attribute the essence to genes: Perhaps it was something in the blood or seeds. This idea is referred to as a placeholder essence (Medin & Ortony, 1989); that is, people believe that there is an essence behind some categories even when they don’t have a specific idea of what it is . . . because there must be one, right?” (p 46)
“Woo-kyoung Ahn and her students at Yale (e.g., Ahn, Flanagan, Marsh, & Sanislow, 2006) have done a fascinating series of studies on how clinicians and laypeople think about mental illness categories. Her work has shown that laypeople tend to think of the categories as more “real” and essentialized than the experts do. They think that there must be something common in people who have a condition, or else they would not all have the same condition. This thing is responsible for their illness. Psychologists who actually treat people are less sure about this. That is, people with borderline personality disorder are somewhat similar, but clinicians also know that they can differ in important ways. And sometimes it is hard to tell whether someone should be in this category or a different one. It is not like trying to tell cats from dogs, nor is there a simple test to find out whether you have a particular condition. So, clinicians often believe that diagnostic categories are to some degree “real,” in that people who are diagnosed with schizophrenia are generally different from those who are diagnosed with bipolar depression, but they also feel that they are categories made up by psychiatrists rather than things that exist in nature. They don’t believe that there is a common cause that explains problems of everyone with a particular diagnosis, unlike AIDS, say, where there is a virus that everyone with the disease has.” (p 88)
Cartwright thought this essentialist view was the definition of “official” diagnosis, but DSM and ICD, which are “official” diagnostic manuals, do not define disorders this way. Experts, of course, have pushed back against this sort of thinking in the field. Which is why she encountered Allen Frances making statements such as “These concepts are virtually impossible to define precisely with bright lines at the boundaries.” It’s funny how people home in on some candid remark by Frances describing psychiatric diagnoses as “bullshit,” but they fail to follow up with how Frances actually understands the nature of diagnostic categories. In a similar way, people often refer to Steven Hyman’s quote that DSM diagnoses are “fictive categories” but fail to take into account how he considers psychiatric disorders to be grounded in human biology but not natural kinds.
The essentialist view of DSM/ICD categories is almost certainly false, but that is not the best way to understand these categories to begin with. Psychiatric categories are a heterogenous mix, like in the rest of medicine. Some appear to be extremes on a continuum (similar to obesity or hypertension), categorizable for practical purposes but without natural discontinuities. Others appear to be symptom clusters, best understood as prototypical categories. And a few seem to be discrete disease entities (e.g. Huntington’s disease or autoimmune receptor encephalitis). Their etiologies are inevitably complex, with psychological development, personality styles, genetics, life stressors, environmental factors (e.g., infections), neuroplasticity, brain circuitry, interpersonal relationships, and sociocultural factors all making an appearance at different levels of analysis.
Cartwright ultimately moves away from seeing her condition as a discrete, treatable illness and starts viewing her mental health problems as products of a complex interplay of personal history, environmental influences, and social conditions. It’s a move in the right direction, certainly, except the problem is that the whole narrative remains distorted by a push and pull with a misunderstood “medical model.”
“How could my illness be like any other, but not definable or testable?... If illness wasn’t the root cause of my suffering, what was?”
How did “illness” come to be treated as a cause? Illness is a descriptive characterization. To call something an illness does not mean we are assuming the existence of a discrete neurobiological disease entity called “illness” that causes it. Illnesses have causes; illness isn’t the cause of anything, let alone the root cause.
This seems to be the primary problem with the discourse around the medical model. The “medical model” is conflated with the idea that all medical conditions are discrete biological disease entities, an assumption that isn’t even true for much of general medicine, let alone psychiatry. When people start off with this understanding, they are rapidly disillusioned, but instead of giving up a distorted understanding of the “medical model,” they end up entirely rejecting the medical approach to mental health problems. And even when they discover that their understanding doesn’t align with how the medical model is better understood, they find excuses to cling on to their disillusionment:
“In academia, psychiatrists will claim that criticising the biomedical model is knocking down a straw man, since they long ago started considering psychological and social factors (what they call a biopsychosocial model). But I’ve seen little evidence of this shift. In England, we’re still five times more likely to be prescribed psych meds than therapy. And the discredited chemical imbalance theory (that depression is caused by a lack of serotonin) is still listed on half of all antidepressant leaflets.”
Ok, but now we are talking about a discrepancy between how the medical framework ought to be understood and how medicine is often practiced in the real world under structural constraints and a scarcity of time and resources. Access to resources matters a great deal… psychiatric medications are often excessively utilized because other modalities are poorly accessible. Once we recognize a discrepancy between theoretical ideals and practical realities, our goal should be to tackle it and understand why the practice falls short of ideal, but our theoretical understanding of the medical approach should be updated to account for the biopsychosocial integrative vision, right?2 Yes, but that is not how critics respond. When confronted with a medical model that isn’t biologically reductive, Cartwright’s response is simply to shrug and keep talking about the medical model as if it were committed to the existence of discrete brain diseases. If the “medical model” is simply a way of talking about all the ways in which the real-world practice of medicine falls short, then we cannot use that to dismiss the theoretical underpinnings of the medical approach to mental health problems.
This is a serious error, one that I see critics make all the time.
First, by giving up existing medical frameworks that seek to address the complex, multifactorial nature of medical conditions and that explicitly recognize the importance of the human experience, critics are forced to clumsily reinvent them without recognizing that this is what they are doing.
Second, by understanding “medical” in this reductive way, they set up medical vs. psychological and medical vs. social dichotomies that are scientifically and philosophically untenable. Trying to purge the “medical” from their explanations leads these critics to make all kinds of ridiculous generalizations about the nature of mental health problems.
So what if OCD is not a discrete biological category? Does it change the clinical reality of Cartwright’s experiences? Does it change the fact that the descriptive diagnostic criteria were a good fit for her symptoms? Does it change the fact that she was profoundly distressed and impaired by her experiences, and was in need of clinical help? Does it change the fact that we have treatments for OCD (medications, psychotherapies, and neurostimulation) that help a large number of people even if they don’t help everyone?
I am not encouraging complacency about essentializing psychiatric categories; what I’m saying is that giving up essentialism doesn’t invalidate our clinical conceptualization and treatment. Unfortunately, various aspects of mental disorder definition and classification are so entangled in the public mind that disillusionment about one rapidly seems to generate disillusionment about the rest.
It is ironic that many people who accuse medicine of presenting an overly reductive and simplistic understanding of mental health problems themselves cannot see beyond an overly reductive and simplistic understanding of the medical model.
Cartwright writes:
“This is what I think is wrong with the medical model: a failure to understand mental health in context. An assumption that a disorder is a “thing” that an individual has, that can be measured, independent of subjective experience. The trauma model can be just as reductive, turning healing into an individual consumer journey and ignoring the environmental conditions in which wounds form. This has empowered professionals to decontextualise distress from the lives of those who experience it; to create pseudo-specific taxonomies of mental disorders. Diagnostic manuals have for decades been giving well-meaning psychiatrists and psychologists the illusion of explaining the suffering of the patient sitting in front of them. This system has hurt none more than those facing social adversity: financial deprivation, poor education, racial discrimination and so on, who are pathologised as though their reactive stress, and not the things to which they’re reacting, were the problem.”
To use this passage as analogical fodder for my meta-commentary, this is what I think is wrong with the popular understanding of the medical model: a failure to understand medical frameworks in the context of the practice of medicine. An assumption that the medical model is a fixed, static ideology that exists independently of the ever-evolving theory and practice of medicine. This has allowed critics to decontextualize the model and divorce it from the experiences of clinicians and patients, creating invalid dichotomies of medical vs. social. And this gives well-meaning critics the illusion of having explained the complex reasons why contemporary healthcare fails so many people.
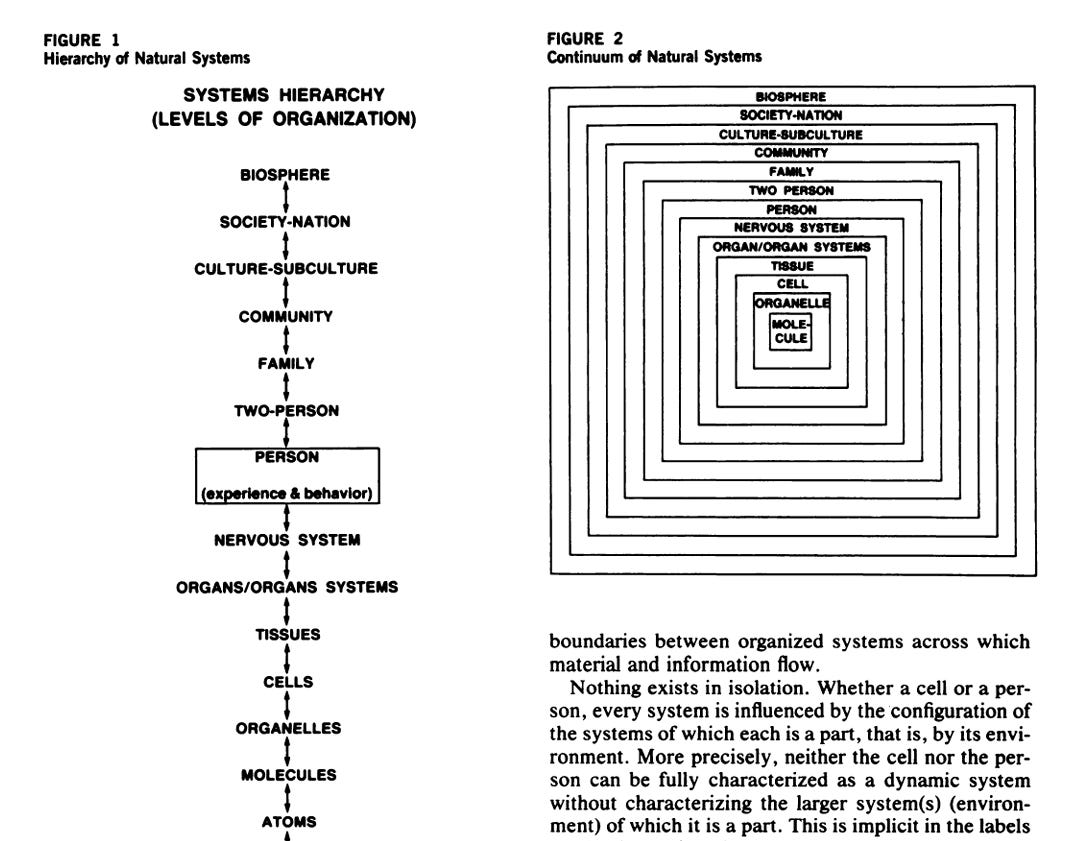
Cartwright talks about “a failure [of the medical model] to understand mental health in context.” It’s easy to demonstrate that this is not the case. The following image is from George Engel’s 1980 paper, “The clinical application of the biopsychosocial model” in the American Journal of Psychiatry.
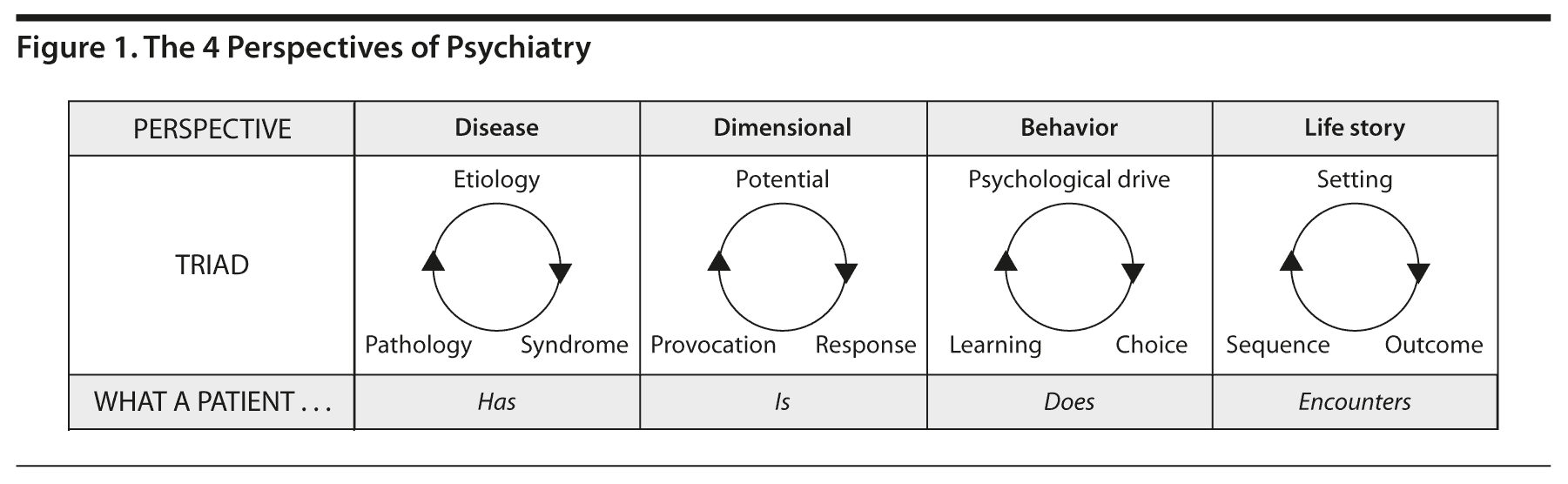
The following figure from a 2012 paper represents the Perspectives approach developed by Paul McHugh and Phillip Slavney (in a book originally published in 1983).
I agree that most medical and psychiatric interventions are focused on the individual, but that is not because the “medical model” fails to understand context, but because the manner in which we as a society organize and reimburse healthcare makes it impossible for clinicians to do anything about the context of a person’s life other than acknowledge its relevance. The clinic often treats individual effects of sociopolitical dysfunction, but the clinic is powerless to treat the sociopolitical dysfunction itself. If we want political change, we have to undertake the difficult, messy work of politics. No model applied in the clinic will do that for you.
It is true that context is often neglected in clinical care, but the point can be easily made without characterizing it as a fundamental deficiency of the medical model. I wrote in a 2023 paper with Ben Druss in JAMA Psychiatry:
“Ultimately, binary distinctions between disordered vs normal distress in the face of stressors, biological vs psychosocial etiologies, and individual treatment vs public health approaches boil down to a constricted and overly narrow view of the medical model. Concerns about medicalization of the psychological lives of youth are triggered by legitimate fears: critics are worried that by conceptualizing distressing responses in psychopathological terms, the relationship to context will be lost or minimized, self-understanding of individuals will be adversely changed, and sociopolitical activism will be replaced by individual medical treatment. Remedying these concerns requires actively emphasizing medical, public health, and policy approaches that take context, self-understanding, and political action seriously.”
“How should these insights inform clinical practice? In addition to treatment interventions, clinical care should focus on conveying an accurate understanding of the determinants of mental health problems to patients and families, including highlighting how social factors may be precipitating, provoking, or perpetuating their symptoms. Enhanced awareness of social determinants of mental health could not only combat the implicit biomedical orientation of contemporary psychiatric care but may also increase support in the general public for relevant sociopolitical reforms and funding for public health initiatives. Furthermore, while symptom rating scales and DSM symptom thresholds are valuable in clinical work, symptoms must be considered in their social context to judge clinical significance and offer treatments accordingly (including judicious use of watchful waiting). While clinicians are limited in their ability to alter social circumstances, they need to use whatever resources are available to intervene at multiple levels, both social and clinical, to help break the vicious cycle between social adversity and psychopathology.”
So, after giving up the medical model, where does Cartwright find answers? Years of therapy with an underground guide under the influence of MDMA and psilocybin.
“At the peak of the trip, I saw a terrifying vision of my mother getting pulled into a colossal black hole in the sky. An image that I then realised represented the cosmic loss I’d felt throughout childhood, as I’d countless times watched her getting dragged off to psychiatric hospital, or drugged into catatonia. When I came round, I was not “cured”, but I had new perspectives. There was never anything wrong with my brain; a fear of separation lay at the core of my problems. An internal stuckness that had never changed, even as I appeared to be flourishing.”
“I did loads of MDMA (ecstasy), both casually and in underground therapy. I meditated. Slowly, a new sense of meaning started to emerge. Having not long ago felt so disconnected that I hurt myself to feel alive, a realisation started to dawn: I am not separate from the world.”
Would Cartwright be disillusioned again if she read scientific critiques of the evidence base for psychedelics? Would she be disillusioned when she learns that psychedelics researchers also talk about psychedelics “rewiring the brain”? Would she be disappointed when she learns that the psychedelic revolution means jack shit for those who experience “financial deprivation, poor education, racial discrimination”?
Is taking SSRIs an act of pathologizing one’s reactive stress, but taking MDMA is to boldly question the medical model?
People pay lip service to the poor and marginalized, scold psychiatrists about scientific evidence, and then go to underground psychedelic retreats where they receive powerful psychotropics that alter their brain activity in dramatic ways, and they come out with some story about “there was nothing wrong with my brain; my OCD was caused by my fear of separation.”
Could the internal contradictions of such narratives be any more apparent?
P.S. I don’t want my defense of the “medical model” (despite my distaste for the term) to be understood as the view that everyone in the mental health field should embrace the “medical model” and think like a physician. I don’t believe that. There is a genuine place for other disciplinary perspectives, and depending on the context and the person, non-medical disciplinary perspectives may be far more helpful. The medical perspective is one disciplinary perspective among many others (various schools in clinical psychology, public health, behavioral neuroscience, social work, neurodiversity, service user movements, etc.) There are advantages (and disadvantages) to viewing psychopathology through a medical lens, and sometimes the advantages are overwhelming and sometimes the disadvantages are. A hegemony of medical language—as has happened, arguably, in public communication—is undesirable. People should have access to and be exposed to a variety of epistemic perspectives. This raises questions regarding when the characterization of a condition as medical should dominate over other characterizations and how competing conceptualizations should co-exist, especially when it comes to competing for public resources (e.g., government-funded healthcare). This issue can’t be resolved simply by appealing to a “biopsychosocial model.” It is a question about hegemony and power, which depends, in part, on the scientific grounding of the fields and the processes by which institutions acquire social legitimacy. More on this in the future.

See also:
Nesse and Stein (2012). Towards a genuinely medical model for psychiatric nosology
Are Critiques of DSM/ICD as Devastating for Psychiatric Diagnosis as Some Critics Seem to Think?
Psychiatric Diagnosis: A Reintroduction
For some reason, this debate seems particularly intense in the UK, which is perhaps why one of the best contemporary explications of the medical model—Ahmed Samei Huda’s The Medical Model in Mental Health (OUP, 2019)—has also come from the UK.
There are serious philosophical problems with the “biopsychosocial model” as it is commonly understood. Scientific explanations of psychiatric phenomena will invariably include variables at multiple levels in some form or fashion, but this recognition by itself is neither a model nor an explanation. The biopsychosocial “model” is nonetheless valuable because it aspires to integrate multiple levels of explanation, and is step towards approaches such as dynamical systems theory and embodied, enactive cognition. See Aftab, A., & Nielsen, K. (2021). From engel to enactivism: contextualizing the biopsychosocial model.
I agree with your article, but less of it coheres with my experience. A Colorado medical school professor as recently as 2022 told me that I have a "chemical imbalance" inside of my brain during a video consult. She is now tenured. A more recent interaction with a PMHNP also stated I have "too much dopamine" and that I could "literally die if you don't take vraylar". (I'm still waiting to spontaneously "die" months later; any day now, sigh).
I believe what fuels much of the disillusionment is that these categories are taught as if they're A). homogeneous, B). static, C). a-contextual, D). overdeterministic or unidirectional. And it's because all of science holds the same assumptions with everything they theorize. E.g. Physicists demand spacetime is perfectly homogeneous, that all "laws" are deterministic, static, and a-contextual and hence generalizable. And when philosophers point out these are instead "first assumptions" the scientist responds with "Well that sounds too philosophical for me so it's not my problem!". Whereas biologists will unapologetically claim nothing living is ever homogeneous, not even "identical" twins, nor are evolutionary processes "purely" deterministic, nor are mutations unidirectional nor a-contextual. Living bodies are also not static (aging is real, circadian rhythms change, values change, habits too etc). And no metabolic process follows a straight line. So why hasn't institutional psychiatry banned these words (homogeneity, static, a-contextual, overdeterministc/unidirectional) yet? What kinds of brains are rising to the ranks of professor to regurgitate these specific assumptions? I disagree it's the general public causing them. Rather, the first time i ever learned of the word homogeneity was in a psychometrics class about "crisply measuring mental disorders", as it were, "carving nature at it's joints".
Thank you for this brilliant discussion. I have become more attracted to psychosocial approaches to mental health problems (e.g., housing, counseling, social supports) over the years and have even seen my daughter benefit from such programs as provided by family members and a local non-profit organization. If my daughter had a place to live in peace with access to food and medical care under a biopsychosocial model, and daily activities to give her life meaning, with friends and acquaintances who accept rather than judge or punish behavioral symptoms by interpersonal rejection or through a carceral system, without guns or other weapons (including those introduced by police officers as first responders), then we might have something approaching a utopian solution for persons with serious mental illnesses. But politicians and members of the public who complain about an over-reliance on medications would reject initiatives to bring such psychosocial supports to scale when they found out they cost far more than pills.