
Rewriting the Grand Plan of Clinical Neuroscience
A Review of “Elusive Cures” by Nicole C. Rust

This is a book review of “Elusive Cures: Why Neuroscience Hasn’t Solved Brain Disorders—and How We Can Change That” (Princeton University Press, 2025) by Nicole C. Rust.
Rust is a neuroscientist and a professor of psychology at the University of Pennsylvania.
Following the success of genetics and molecular biology, molecular neuroscience became the dominant way of thinking about psychiatric disorders in scientific circles in the last decades of the 20th century. This thinking is illustrated well in Eric Kandel’s 1998 paper on an intellectual framework for psychiatry, and it casts psychiatric disorders as disorders arising from genetic and molecular cascades. It pictures mental illness as the outcome of a domino chain: genes shape proteins, proteins shape neurons, neurons shape circuits, and disrupted circuits manifest as mental dysfunction. Kandel’s formulation also recognizes that environment and social factors play a role but conceptualizes them as feeding back into the domino chain via gene expression and brain wiring so that nurture becomes nature through learning and development. Both psychotherapy and medication, within this view, alter brain function by modifying gene expression and neural circuits. This approach led to an explosion of neuroscientific research and an expanded understanding of the brain, yet it also narrowed how we think about mental disorders scientifically and how we go about researching potential treatments.
It was obvious by the 2010s that basic research in neuroscience and genetics had not translated into new clinical treatments that meaningfully improve clinical outcomes. Hopes that neuroimaging research would provide clear biomarkers for mental illness had not yielded robust, clinically actionable results. Brain activity patterns differed across individuals and often failed to replicate, such that no neat correspondence could be discovered between psychological categories and brain functioning. Gene expression patterns and isolated measures of brain activity provided inadequate explanations. This prompted a great deal of commentary and handwringing. Some critics went so far as to dismiss neuroscience as a scientific dead end in psychiatry, viewing it as irrelevant to understanding the nature of mental health problems. Psychiatric discourse was caught, in the words of Steve Hyman, in a “familiar dialectic between overclaiming and moral outrage over brain biology.” Psychiatric researchers and scientific leaders became acutely aware of the need to play a scientifically well-grounded long game that avoids the kinds of reductive and overconfident claims that had been made in the past.
My psychiatric training was in the mid-2010s while this conceptual transformation in neuroscience was taking place. The neuroscience I encountered during psychiatric training bore a distinctly reductionistic flavor. The emphasis was on the search for neurological correlates: which neurotransmitter aligns with which symptom, which brain regions are associated with which clinical presentation, which circuit is disrupted in which disorder, etc. It was productive in its own way but ultimately limited in what it could accomplish. Later, guided by the writings of public-facing scientists such as Lisa Feldman Barrett, Anil Seth, Mark Solms, Luiz Pessoa, and Karl Friston, I stumbled onto the new intellectual landscape of neuroscience, one that emphasized the complex, dynamic, computational, predictive, and enactive characteristics. The new language was one of feedback loops, information processing, and embodied cognition. The difference was striking.
Nicole Rust’s Elusive Cures is an insider’s account of how contemporary neuroscience is tackling the failures of the bench-to-bed pipeline and how neuroscience is moving away from the molecular-genetic framework to a new grand plan that understands the brain as a complex, dynamic, computational system. Rust is a brilliant, accomplished, thoughtful, and philosophically and clinically informed neuroscientist, and it is a treat to see her make sense of this terrain. The end result is an accessible book that is deeply intelligent and informative.
This is a simplification, but Rust discusses that the translational strategy of molecular neuroscience had been cashed out as follows:
Identify a gene linked to a disorder.
Create an animal model (often a genetically altered mouse).
Study how the mutation disrupts brain function.
Develop a drug to fix the problem.
Translate findings to humans through clinical trials.
This was captured in the phrase “one gene, one drug, one disease.” However, most brain disorders cannot be traced to single genes or even small groups of them. Disorders like schizophrenia, depression, or Alzheimer’s are highly polygenic with complex etiologies with developmental and environmental influences, making the approach unrealistic. Rust notes that simplification is inevitable in science (the familiar adage—all models are wrong but sometimes useful—makes frequent appearances). The problem is that molecular neuroscience oversimplified the brain in a way that was not only wrong but also unhelpful.
Rust understands the brain as a “complex adaptive system that computes.” That is, the brain’s behavior doesn’t come from isolated parts but from interacting components linked by feedforward and feedback loops, so key properties (and problems) emerge from their interactions rather than from a single node or pathway. “Adaptive” points to homeostasis and allostasis—the brain continuously predicts needs and adjusts internal setpoints via feedback to keep the organism stable while responding to change. Because of this architecture, brains are robust yet fragile and often operate near a critical ‘edge of chaos,’ where small nudges can push dynamics toward dysfunction (e.g., coma or seizures) or back to healthier regimes. “Computes” retains the information-processing idea that the brain carries out algorithms or computations on representations.
She writes:
“What I affectionately refer to as the Grand Plan for brain research is a description, in broad strokes, of how we’ll go about finding the causes of brain dysfunction and develop treatments. My own journey with this book began with the realization that I could not write down a Grand Plan for brain research that I was optimistic about—one that could describe how we plan to go from where we are now to new therapies. I knew the sketch: figure out the causes of brain dysfunction and create treatments. But what is the plan to accomplish that? What I knew was that the way the plan was formulated in the 1990s and depicted in popular textbooks (like find a gene, make a mouse, create a drug) wasn’t going to work. It took me the better part of 2 years to sift through the history, philosophy, and science required to see the emerging alternative, and at times it was overwhelming. But the act of writing it down helped me understand what the new and promising Grand Plan for brain research is. Now that I can see it, I’m optimistic and grateful to know it.” (p 223)
In an earlier post I had commented that “brain disorder” talk indicates a commitment to a neuroscientific research program that can be both virtuous and non-virtuous. Rust’s approach is very much of the virtuous variety. She relies on the “brain disorder” framing partly because she is working within the neuroscientific tradition and partly because it provides a unified framing for both psychiatric and neurological disorders. But she is aware of the limitations of understanding psychiatric conditions as disorders as well as understanding them as brain disorders. (The focus of my review is on psychiatric disorders but Rust also extensively talks about neuropsychiatric disorders such as Alzheimer's and Parkinson’s disease.)
In characterizing them as disorders, she’s driven primarily by a concern for suffering. In the author’s note, she clarifies:
“I acknowledge that there are complexities around whether and when we should consider some conditions as "dysfunction" as opposed to a type of neurodiversity that society has wrongly become intolerant to—cases of autism, attention deficit hyperactivity disorder, and depression are all examples. That said, for each of these conditions, a subset of diagnosed individuals suffer in ways that can benefit from treatment. For those individuals, when our existing treatments fall short, we need better ways to help them. With this empathetic spirit, I use the terms “dysfunction” and “disorder” to refer to the conditions of individuals who need better solutions than the ones we can offer them today.” (p xi)
And with regard to calling them brain disorders, she notes:
“The commonly held position among researchers is that neither the brain nor the mind will be the singular best way to explain the causes of mental disorders or think about interventions. Neither the term “mental disorder” nor “brain disorder” is thus a great fit to describe these disorders (because these disorders involve not just one but multiple levels). The most critical, nuanced question we need to focus on is where the emphasis should be placed for any specific disorder—or even a specific individual.” (p 110)
Is the brain a computer? Rust emphasizes that this idea can function as a reality, metaphor, or model depending on how it is framed. In a philosophical sense, the brain could be seen as a literal computer, and its functioning can be recast in computational terms, though this is often too broad to offer any specific guidance. More commonly, researchers adopt the metaphor of the brain as a sequential computer, processing input into output through modular computations such as vision, memory, and decision-making. When formalized into testable predictions, the idea becomes a model, enabling mathematical and computational representations of brain function.
Rust explains David Marr’s three levels, computational, algorithmic/representational, and implementational—recast by Rust as why, what, and how—as complementary ways of approaching explanations of brain functions. The why-level is about the problem to be solved and the goal of the computation. For example, in vision, the why-level asks why the brain needs to identify a face and what counts as a good strategy to achieve that. Behavioral descriptions typically fall at this level. The what-level focuses on what computations the brain performs. In the case of vision, this means describing the step-by-step computations different brain areas carry out to construct a neuron that selectively responds to a face. Rust highlights this level as a kind of “bridge,” because it connects the biological mechanisms (how) with the higher-level goals and behaviors (why). The how-level concerns the biological implementation: the neural circuits, specific neurons, and molecular cascades that make those computations possible.
As an illustration, Rust uses Marr’s levels to explain how Ritalin improves attention in neuroscientific studies. At the why-level, behavior is studied through tasks like change detection, where people perform better when they attend to a cued location, and Ritalin further boosts this performance. At the what-level, attention reduces “noise” in internal brain signals, making stimuli at attended locations more distinctive, and Ritalin enhances this noise reduction even more. At the how-level, the mechanism is thought to involve the prefrontal cortex increasing norepinephrine, which strengthens feedback to the visual system and decorrelates neural noise. Filling this “what-level” gap is crucial, as it allows us to connect biology with behavior and dysfunction in meaningful terms.
At the same time, Rust realizes that understanding the brain as a computer and seeking integrated multi-level explanations is incomplete on its own.
“Until I sat down to write this book, I also presumed that filling in the what-level gaps between the why and how levels would be sufficient. I no longer think that’s the case. I suspect that by regarding the brain as a (sequential) computer, we’ve set up the problem in the wrong way insofar as our goal is to understand and treat brain dysfunction. The brain as a computer is an extension of the domino chain, and that’s neither the type of thing that the brain is nor why it breaks. Multilevel understanding is part of the answer but not the entirety of it. The puzzle needs one more piece.” (p 113)
The missing piece in Rust’s view is understanding the brain as a complex, dynamic, adaptive system.
Researchers have begun developing preliminary mathematical equations that govern mood (and do a half-decent job at predicting empirical results) based on experiments in which subjects gambled for rewards and report their happiness. These models show that mood depends less on total rewards and more on unexpected gains and losses, with recent events weighing more heavily than older ones. In a gambling experiment, for example, an equation predicting mood looks like
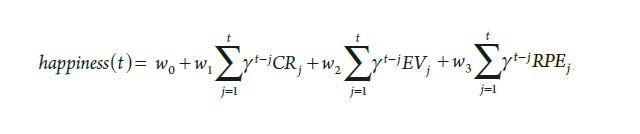
where CR refers to certain rewards, EV to expected value, and RPE to reward prediction error.
This research work suggests that mood changes are driven by prediction errors. While mood is adaptive, helping organisms learn about changes in their environments, it is also fragile, since repeated negative surprises can create self-reinforcing downward spirals characteristic of depression.
“If we expect things to happen and they do not, reward prediction errors build up. When the things happening are unexpectedly good, we become happy; in contrast, when things are unexpectedly bad, we become sad. And it turns out that this sadness is transformed into the perception that outcomes are worse than they actually are. This makes mood profoundly fragile because it can get stuck in a negative feedback cycle where bad moods lead to the distorted perception of bad outcomes, which in turn leads to worsening mood.” (p 131)
Complex adaptive systems, Rust observes, are designed to be robust, but that very robustness introduces fragilities. The immune system, for example, protects us by adapting to pathogens, but occasionally that adaptability misfires, producing autoimmune disorders.
Experiences and behaviors are notoriously difficult to measure. Measurements depend on definitions, and here the field falters. There is a circular problem: to measure these concepts we need understanding, but to gain understanding we need measurements. To tackle this, Rust turns to the history of measuring temperature. Early scientists developed thermometers long before they understood molecular motion or heat transfer. These instruments allowed systematic study, which in turn enabled later theories. Neuroscience, she suggests, needs analogous strategies of creating usable measures of mental phenomena without requiring complete theoretical understanding from the start.
Epistemic iteration is the “try something, then refine it” engine of scientific progress: when you don’t yet truly understand a phenomenon, you start with your best workable definition and measurement, use it, learn from its limits, and iterate until both a solid measure and an explanatory theory emerge.
In Rust’s vision for a new neuroscience, epistemic iteration is the practical way to make headway on emergent, hard-to-define brain phenomena (like mood, depression, or consciousness). It legitimizes imperfect early models and measures as necessary stepping stones, frames progress as successive refinement across generations, and cautions against getting stuck in “local minima” when the first guess is very off-base. Epistemic iteration allows for coordinated top-down and bottom-up efforts, beginning with usable, theory-agnostic measurements of complex states while also developing mechanistic accounts, iterating both until they converge.
Causation in complex systems is also not straightforward: many influences interact across levels, timescales, and contexts. Rust goes into philosophical debates about causality itself and distinguishes between two different kinds of causes: causal production, a notion of causation where one thing generates or directly brings about another, and causal dependence, where anything that can affect an outcome (i.e. anything that can potentially be a target for intervention) can be considered a cause. In neuroscience, both types are relevant, yet often confused and conflated. Rust argues that in complex systems, instead of asking whether something is causal, we should focus on how different causal influences interact. To do this, researchers need to build mechanistic models that select relevant influences in a useful way rather than exhaustively document any and all causal influences.
Rust draws on examples from chaos theory and weather systems. Complex systems can operate in chaotic regimes, where tiny changes have vast, unpredictable consequences. Just as meteorologists avoid trying to redirect hurricanes, neuroscientists must recognize that attempts to push on one neural pathway can cascade in unexpected ways. Even when a system is not fully chaotic, its interdependence makes control extremely difficult. Treatments cannot simply achieve change; they must achieve the right change with minimal side effects while avoiding the adaptive responses that produce treatment tolerance.
Rust develops the weather analogy to reframe how we think about treatment, prompting the question of whether influencing seizures or psychosis is any easier than steering hurricanes. In meteorology, first came prediction, with detailed and increasingly accurate forecast models; then came attempts at control. Forecasting succeeded while control largely failed, as decades of cloud seeding and storm-modification projects collapsed due to the difficulty of the undertaking and undesired changes in the trajectories of hurricanes. Applied to the brain, this means that therapeutic nudges can reverberate unpredictably, producing side effects or treatment resistance. Yet Rust notes that there is a crucial disanalogy: unlike weather, the brain contains self-organizing, stabilizing loops that often bring seizures or mood episodes to a spontaneous end, offering levers that might be clinically harnessed.
Rust reflects on the difficulty of explaining these ideas in a condensed, pithy manner:
“OK, that’s great, but what’s the new analog of “find the broken domino and fix it”? What’s the new version of “find a mutated gene, make a mouse, create a drug”? Or “find a brain area with aberrant activity and stimulate it”? The challenge is that complex systems resist pithy phrases because they don’t fail in ways that are as easy to describe. The cause could be a broken node, an aberrant set point (due to the strength of interaction between nodes), or something else that leads an emergent property to change. The new Grand Plan can’t be captured more succinctly than “create and test models of the brain as a complex adaptive system to infer fragility and determine control.” The phrase launches from the presumption that we have a way to characterize dysfunction via some type of measurement. It emphasizes that the goal is to create a complex dynamical systems model to figure out the causes of the disease (fragility) and how to restore health (control).” (p 231)
Over the past one to two decades, psychiatric classification, psychiatric genetics, evolutionary psychiatry, psychiatric neuroimaging, and psychopharmacology have all undergone transformations because of better appreciation of scientific complexity. Elusive Cures shows how dismissals of neuroscience by mental health professionals on grounds of explanatory reduction and disease entity assumptions are outdated. The new neuroscience presented by Rust is humble, mature, and pluralistic. Readers who lived through the scientific arrogance of the Decade of the Brain may find it difficult to let go of their distrust, but if they are open-minded, I would strongly encourage them to pick up the book. Mental disorders are complex enough that no single discipline can claim the full scientific story. We do not yet know the limits of the neuroscientific project of building a bottom-up language to explain psychopathological phenomena. Time will tell, but I finished Elusive Cures with a renewed sense of scientific optimism.
See also:



Awais, I was disappointed that you did not respond to my comment last week. After a week's thought, I think my point still holds. Psychiatrists hardly ever see their patients for prolonged periods, so they never have direct experience with the reality that the same med will work very well for some and be very detrimental to others. Psychiatrists have less of a chance to see the pros and cons of a treatment.
https://www.psychiatrymargins.com/p/why-has-critical-psychiatry-run-out/comment/155705496
Once again, an approach to psychiatry that is hyperindividualistic, and rooted in the computer model. But humans are not fundamentally individualistic, we begin life as a dyad (mother-infant) and the quality of that dyad is literally of life and death importance. We continue through life as nodes in a web of relationships, with our moods, behaviors, and thoughts profoundly shaped by this web. WE value connection and relational warmth in the web more than we value alleviation of our suffering. Clients are willing "to receive an intervention that had a lower recovery rate by 38.14% to ensure that they received a therapist with whom they
could develop a positive working relationship. " JOURNAL OF CLINICAL PSYCHOLOGY, Vol. 66(12), 1217--1231 (2010). Until theories of mental health/disorder start from perspective of the relationships between people, they will be woefully incomplete, giving into the reductionism of science, rather than the social web that weaves us together from infancy to death.