
Vice and Psychiatric Diagnosis: A Discussion with John Sadler
Recognizing and reversing the exclusion of vice from psychopathology

John Z. Sadler, MD is Professor of Psychiatry and the Daniel W. Foster, M.D. Professor of Medical Ethics at the University of Texas Southwestern Medical Center. He directs the Division of Ethics in the Department of Psychiatry and is the institution-wide Director of the Program in Ethics in Science & Medicine at UT Southwestern. Sadler is one of the founders of the Association for the Advancement of Philosophy and Psychiatry (AAPP), as well as the International Network of Philosophy and Psychiatry (INPP). He maintains a video archive of philosophers of psychiatry, www.psagacity.org, which offers in-depth, high-definition video interviews of notable scholars in this field.
He is the immediate past editor-in-chief of the journal Philosophy, Psychiatry, and Psychology and is a co-editor of the Oxford University Press (OUP) book series, “International Perspectives on Philosophy and Psychiatry,” the latter currently spanning over 50 volumes. In addition to numerous books he has edited or co-edited, Sadler is the author of the comprehensive and seminal monograph, Values and Psychiatric Diagnosis (OUP, 2005). A collaboration with philosopher Jennifer Radden, The Virtuous Psychiatrist: Character Ethics in Psychiatric Practice, was published by OUP in 2010. In 2024, OUP published his most recent book, Vice and Psychiatric Diagnosis.
Awais Aftab, MD, is a clinical assistant professor of psychiatry at Case Western Reserve University. He is interested in conceptual and philosophical issues in psychiatry and is the author of this Substack newsletter.

Vice and Psychiatric Diagnosis (OUP, 2024) by John Z. Sadler is an ambitious exploration of the intersection between psychopathology and immorality, offering a fresh intellectual history that spans centuries. Sadler tackles the neglected but important question of why some mental disorders are “vice-laden” (involving criminal or immoral behavior), while others are not, and this line of inquiry serves as a springboard for addressing profound questions about how we define and respond to mental illness and criminality. It leads Sadler to identify and challenge “a pervasive, powerful, and inconsistent set of assumptions about how key aspects of reality are organized in Western culture and our collective minds.”
Sadler’s approach—a variety of philosophical anthropology—is unique in its scholarly depth and interdisciplinarity, incorporating insights from medicine, psychology, philosophy, history, law, criminology, public health, and social policy. Our current struggles with placing disturbances of moral conduct within psychiatric nosology have deep historical and social roots. The book concludes with forty theses that summarize main arguments, tease out implications for philosophical analysis and clinical practice, and suggest ways forward for institutional change and public policy reform.
Abbreviations:
CMC: Complex multicausal
FM: Folk-metaphysical
HiTOP: Hierarchical Taxonomy of Psychopathology
NGRI: Not Guilty by Reason of Insanity
RDoC: Research Domain Criteria
VMDR: Vice and mental disorder relationship
VAPD1: Values and Psychiatric Diagnosis (2005)
VAPD2: Vice and Psychiatric Diagnosis (2024)
Some quotes from Vice and Psychiatric Diagnosis:
“The peculiar bundle of contradictions which describes the current VMDR is, in large part, a cultural artifact of prevailing conflicts and incompatibilities between complex multicausal (CMC) scientific metaphysical assumptions and Abrahamic folk- metaphysical assumptions. These conflicts of assumptions manifest themselves in contrasting views of reality, pertaining to the classification of psychopathology, the practice of forensic/ correctional psychiatry, to criminal law, to criminal justice and penology, and even to other social welfare institutions like care of mentally ill and intellectually disabled people, and juvenile justice concerns…
Vicious conduct may, or may not, be disordered. In the former it should be investigated, characterized, with treatments developed, tested, and implemented. In the latter account, nondisordered vice conditions should be treated as a challenge for civil societies to develop effective and just social welfare responses…” (p 486)
“What underlies such potential controversy is the frequent absence of the social structures that provide humane rehabilitation, on the one hand, and powerful fears that reform will leave holes in public protections from crime, on the other. These fears are legitimate— I hold them myself. However, their realization is not inevitable…” (p 487)
Aftab: I want to begin by saying how much I admire you. You are a great role model for junior scholars, especially psychiatrists drawn to the ethical, historical, and philosophical dimensions of our field.
When I first read your 2005 book Values and Psychiatric Diagnosis, I thought it was brilliant, and when I started Vice and Psychiatric Diagnosis earlier this year, I honestly wondered if it could live up to its predecessor. But you exceeded every expectation! It’s a remarkable work whose significance will, I think, only deepen with time. The scholarship in Vice and Psychiatric Diagnosis feels like the kind that opens entirely new fields of inquiry through the sheer force of rigor and innovation. I wouldn’t be surprised if, a century from now, it’s seen as a landmark book that transformed our understanding of vice and psychopathology. This may sound hyperbolic to readers, but it’s my measured assessment!
When I began reading it, I wasn’t quite sure what to expect. I anticipated that it would complicate the ‘mad versus bad’ distinction, but I didn’t know how, and I thought that perhaps you will make an effort to distance psychiatric nosology from vice-laden concepts. What I didn’t expect was the bold direction you took—embracing rather than rejecting vice-laden mental disorders—and the far-reaching implications of doing so.
You’ve mentioned that your working viewpoint on the issues involved was completely transformed in the process of researching and writing the book. Can you say more about what sort of direction you had in mind when you started and what led you to rethink your basic assumptions?
Sadler: Awais, having you give such a close read of my book and ask such perceptive and insightful questions is a joy and a privilege, so thanks for this. Some minor bookkeeping before I start. For brevity’s sake and to avoid confusion, I refer to Values and Psychiatric Diagnosis (2005) as VAPD1, and Vice and Psychiatric Diagnosis (2024) as VAPD2.
Regarding your first question, how did I start and how did I change, I can mention our colleague Diogo Telles Correia, a philosopher of psychiatry and clinician at the University of Lisbon, who asked me a similar question. After my talk at the International Network for Philosophy and Psychiatry meeting last year in Vienna, Diogo came up to me and recited chapter and verse from VAPD1 about how I had problematized the issue of ‘vice-laden disorders’ in that book. Back then I was concerned about psychiatry in a ‘police’ function, among other things, and that having vice-laden disorders encoded in the DSM blurred this boundary between policing and doctoring. The simple idea here was that policing is inappropriate to ethical doctoring, so having vice-laden disorders was a problem needing to be expunged from our diagnostic nomenclature. However, Diogo noticed in Vienna that I seemed to have changed after hearing my Vienna lecture about psychiatry and the problem of vengeance. He, and you, were right that ‘I have changed’. I have changed my viewpoint in the directions we discuss below and appear in the book.
When I started after VAPD1 came out, I was mostly worried about the policing/doctoring problem, but thought the most important first step was to explore the paradoxes about vice and mental disorders in psychiatric practice and as illustrated in some DSM categories. I noted that I define ‘vice’ in this context as wrongful and/or criminal conduct. Exploring the paradoxes of vice-laden disorders in the DSMs led me to the need for an ‘intellectual history of madness and morality’ endeavor for chapters 4 and 5. Early on with that historical effort, I realized that the policing/doctoring dichotomy is relatively new in Western history—wrongful/immoral conduct has been commingled with madness since prehistory up to the 16th century. That is, sin and madness were commingled. Not until the late medieval-early Enlightenment era did our modern concept of ‘crime’ crystallize into the idea of ‘offenses against the public.’ This new, modern notion of crime separated the notions of sin/crime from the then-new medical concepts of mental illness. It’s a complicated story with many twists and turns and was fascinating to develop for the book.
At risk of editorializing with your question, I am convinced that doing rigorous and fair-minded philosophy can result in changing one’s opinion and position on things—further, I think doing rigorous and fair-minded philosophy results in bona fide discoveries of comparable significance to scientific discoveries. The process of writing this book provides several examples, perhaps one of the most significant ones being that rather than eliminating vice-laden disorders, we should assimilate them into our tasks of helping people flourish.
Sadler: I think doing rigorous and fair-minded philosophy results in bona fide discoveries of comparable significance to scientific discoveries. The process of writing this book provides several examples, perhaps one of the most significant ones being that rather than eliminating vice-laden disorders, we should assimilate them into our tasks of helping people flourish.
Aftab: You’ve worked on this book for twenty years or so. This kind of dedicated patience is perhaps somewhat outdated these days (and unfortunately so). Someone starting on a project like this today would probably publish a series of academic papers over several years, give numerous talks, and maybe even have a blog or newsletter devoted to it. But reading Vice and Psychiatric Diagnosis, I can see the merits of this kind of sustained, careful, rigorous scholarly work that is conducted with patience and then published in a coherent, unified way. For junior scholars reading, what would you say about your style and philosophy of scholarship?
Sadler: I was amused by your use of ‘dedicated patience’ in reference to the VAPD2 (Vice and Psychiatric Diagnosis) project. Writing VAPD2 was not about patience and dedication, but about passion and opportunity. Being able to read, research, and write on this was the kind of fun that is its own reward—much akin to the thirst to paint artists describe when they can’t do their work. However, it wasn’t always that way for me. When I was a new faculty member in my 30’s, I liked Gloria Steinem’s quote about writing: “I don’t like writing, but I like having written.” That was true for me at the time, but after about 10 years I found the writing not just likable, but a positive feature of my life and mental health.
The process of developing VAPD2 was kind of old-fashioned; the ‘lone scholar laboring with his books by candlelight within the tapestry-hung study.’ Ha! It wasn’t entirely like that, and the work spanned a transformational time in scholarship. I’m old enough to remember doing scholarly background research in a physical library as a high school student, chasing down books using a ‘card catalog’, and making notes on index cards for my paper. By the time I worked on VAPD1, I was able to make photocopies instead of index cards, a great advantage, and I tracked the development of DSM-III and IV drawing from the APA archives in Washington, DC. By then I had a USB portable scanner and a laptop. It was fun. But by the time of VAPD2, Google was well into the process of digitizing (supposedly) all books. The result was that I could read Benjamin Rush and Isaac Ray from Google scans in the comfort of my office and computer. This made it feasible to do the ambitious work that you note regarding the historical chapters. Otherwise, I would still be chasing down books and papers in physical libraries! I did do a bit of what you envision as today’s process; problem areas that I wanted to explore in more detail would lead me to write chapters and articles for others that then would allow me to cite and abbreviate my discussion in VAPD2. Presentations at meetings would allow me to explore others’ reactions to this or that thread of my thought.
This doesn’t address though the idea of commitment to a big project like VAPD2. I think this is also related to my personality and interests. I mention in the book how much I like the ‘wow factor’ in my own nonfiction reading; few things for me are more rewarding than a transformative insight gained through reading. (Indeed, I find myself impatient with the now-ubiquitous passion for videos; I want them to skip to the good stuff, the ideas!) However, another aspect about me and writing is that I love the exploration and discovery, particularly that a simple question like “Why do we have these vice-laden disorders and not others?” can open the doorway into a world of interconnected histories, concepts, and mysteries. Hence the mention in the introduction that the process of writing VAPD2 was like a detective pursuing a whodunit in crime fiction, though I was pursuing a ‘whatdunit’. A third element is that I like the big questions, partly because I think they are more important, partly because they are too-often neglected in academia and science, and partly because they are more motivating and compelling for me. I have worked in my academic medical institution and had a more-or-less conventional academic psychiatry career in teaching, practicing, and researching, enjoying all of it. However, my time for research and writing was always limited, grant funding was scarce to unheard of, and other duties called and still call. I recall Norman Sartorius’ famous quote about academic success needing three things: “time, money, and ideas, and rarely do all three come together.” In my case, ideas were easy for me, time and money were the challenges.
Implicit in your question is how I might advise junior scholars. Perhaps some of the above responses imply some advice. For clinicians that want to do philosophy/psychiatry scholarship, they must be flexible in finding pathways to realizing their interests. It’s easy to say ‘do what you love’ but this is always tempered by realities of financial support, or lack of it, other obligations to people and institutions, and personal aspects—one’s aptitude, interest, energy, family, health, etc. Perhaps I should advocate for patience and passion with a pragmatic attitude.
Aftab: In order for us to treat morality as a “faculty” (a word we don’t encounter as much in medicine these days!) in psychology and psychopathology akin to affect and cognition, with corresponding functional and dysfunctional states, I imagine that we need a naturalistic and scientific account of morality. Or at the very least, we need a way to talk about and study morality and its disturbances in naturalistic (i.e., complex, multicausal) terms. Has the scientific study of morality advanced to a degree that we can replace Abrahamic folk assumptions in clinical and legal work? Is ‘Moral Psychology’ the field we should go to for guidance in this regard?
Sadler: We were at only volume 3 of Philosophy, Psychiatry, & Psychology (1996) when we published Jennifer Radden’s account of ‘Kantian faculty psychology’ in psychiatric categorization. Jennifer articulated the roots of the ‘faculty’ approach in the parsing of mental functions, which persists, for better or worse, today through segmenting the mind into cognition, conation (motivation), and affection (emotion). These functions have sedimented into our ordinary language and our ways of thinking even in the face of molecular biology and RDoC neural pathways. Back in Kant’s time the capacity for moral experience and function continued to be mystified into some presupposed Abrahamic domain that somehow didn’t belong with the other faculties. This mystification of morality is a great example of the epistemic power of folk-metaphysical assumptions; not only are they taken for granted, they structure our perception of reality and are imbricated (built into) our institutions, as in the case of Abrahamic morality through criminal law and religious traditions and worldviews. As the history chapters in VAPD2 describe, alienists and the later psychiatrists always had scientific interest in wrongful conduct and immorality; it’s just been haphazard and wildly incoherent. 18th- and 19th-century alienists had ‘homicidal insanity’, and we’ve had the concept of psychopathy for at least a century. This has been changing though since the late 20th century. I just did a PubMed search on ‘psychopathy’ with 1399 pages of hits. Compare this with ‘antisocial personality disorder’ with 1245. Psychopathy turns out to be a great example of a morality-entangled psychopathological concept in VAPD2. It’s only our stubborn metaphysical marginalization of wrongful conduct that frames scientific inquiry into it as somehow remote or illegitimate.
Regarding ‘replacing’ Abrahamic folk-metaphysical assumptions (free will, individualism, personal responsibility, just deserts) in clinical and legal work: I don’t see this dependent upon scientific understandings so much as dependent upon the public will to accept that retributive (punishment-oriented) justice is not just ethically problematic but ineffective in crime prevention. The evidence for the latter is reviewed in chapters 6 and 7.
If we see immorality and criminality as just another kind of human problem, the science can grow in proportion to the other ‘faculties.’
Aftab: You start off with the question, “Why do some categories of mental disorders involve value judgments of immorality and criminality, while others do not?” Your answer to this question by the end of the book looks something like this: there are in fact legitimate disorders of moral conduct and given the existence of such disorders, we should expect that some categories of mental disorders will inevitably refer to immoral and criminal conduct.
You write:
“Under CMC accounts, people act wrongfully under complex interactions with environment, personal history, and personal biological endowment.” (p 495)
“The mad- versus- bad debate should disappear as an artifact of the cultural confusions regarding the CMC and Abrahamic FM [folk-metaphysical] accounts of the person.” (p 495)
“Szasz wanted wrongful conduct, whether mad or bad, to be handled by institutions like the criminal justice system, education, and religion. Only bona fide diseases, with pathological somatic findings, warranted medical interventions.
In contrast, my account collapses the mad- versus- bad debate in a different way. If we set aside Abrahamic metaphysical assumptions and admit vice behavior as just another kind of human problems worthy of scientific understanding, treatment, and prevention, then ‘bad’ points to domains of experience and behavior that can be pathological like any other domain. The historical stigma and neglect by medicine and psychiatry can be corrected through a collaborative paradigm between psychiatry, the social sciences, neuroscience, criminology, and ‘neurocriminology’.” (p 496)
What would you say to contemporary critical psychiatrists who want to hold on to the dream that we can, and we should, cast out all references to vice from our diagnostic criteria?
Sadler: So far, I haven’t heard from contemporary critical psychiatrists about my book, though that’s no criticism of them—it’s too new. My take on this group is that they are heterogenous in their viewpoints and their relationships with service-user groups and other advocates and critics of mental health. At least as articulated by Middleton and Moncrieff’s overview from 2018 (Br J Psych Advances), critical psychiatrists admit to the need for coercion when individuals are overwhelmed in dangerous or intolerable situations, much like I do, though my sense of justification for coercion has to do with protecting the public from people who cannot otherwise be contained and aided more humanely. What these folks share relevant to VAPD2, I think, is a liberatory interest in people oppressed by unjustified/unjustifiable sociomedical constraints. In my case, we should add unjustified/unjustifiable penal constraints. Without addressing critical psychiatry explicitly, I go to considerable trouble in the final chapters in (a) sketching out requirements of a just, democratic society such that (b) incorporating wrongful/criminal conduct that fulfills rigorous requirements to qualify as ‘disordered’ into psychiatry results in (c) less punishment, less coercion, and a more-just, more liberatory treatment/rehabilitation. I also say these just-society requirements are currently not met in Western democracies, though some nations are [much] better at it than others (the U.S. not among them). Moreover, the looming growth of authoritarianism around the world makes my vision of mental health and criminal justice reform all the more daunting. After two decades of consciousness-raising by our critical psychiatry and service-user colleagues, I worry that the potential for psychiatric abuse is growing, not shrinking. I’m ‘speaking out’ in the book.
Sadler: After two decades of consciousness-raising by our critical psychiatry and service-user colleagues, I worry that the potential for psychiatric abuse is growing, not shrinking.
Aftab: You advocate for developing “spectrum or graded accounts of blameworthiness/wrongful action for moral and criminal offenses,” but you also make a case that “For vice-laden disorders, replace concepts of ‘responsibility’ with regulation of extreme behaviors, when applicable.” How do you reconcile the two?
Sadler: Awais, you have astutely zeroed in on an issue that I felt the need to acknowledge, but mostly set aside in that it would take me on another long pathway of analysis which would make a very long book even longer. It indeed demands a book unto itself. The problem you have raised with these questions is how to translate the notion of Abrahamic ‘personal responsibility’ into CMC folk-metaphysical language for practice/research, the latter aimed at dispensing with Abrahamic blame and vengeance. This issue requires the kind of ongoing collaborative research between (particularly) the philosophy of psychiatry and the relevant sciences, but also more philosophical attention to accounts of free will and causality.
To give your readers a taste of the problem from my vantage point, we can think about some seemingly simple causal relationships that result in problematic behavior. Consider individual A with a genetic inborn error of metabolism and is disinhibited and aggressive as part of their syndrome, leading to his striking of caregivers. A second example is that individual B works a 24-hour shift, falls asleep at the wheel on the way home, and hits a pedestrian, injuring them. We intuit in these cases that the first one, A, has less ‘responsibility’ in Abrahamic terms, and has more robust, and perhaps fewer, causal vectors shaping A’s aggression than in individual B. B, we can intuit, is situated in a more complex, multilevel, causal network of vectors: the unreasonable schedule at work, the need for B to keep this job, the background of sleep debt developed by B over the prior weeks, the distractions of heavy traffic, on down to the neurobehavioral mechanisms of sleep regulation and such. In the legal Abrahamic FM context, both A and B are ‘responsible’ for the adverse result, though the courts may be more likely to ‘excuse’ A. Under the CMC FM context, we need a method for weighing the relative contributions of the causal vectors, and quantifying their ‘weights’, e.g. the genetic error in A likely has more ‘weight’ in causation than, say, how much of a sleep debt B has, or the employer’s causal weight through setting unreasonable shift durations. All the vectors may be causally relevant, but how to parse them in addressing the harms associated with A and B’s cases is a conceptual and practical challenge. Several of our friends in philosophy of psychiatry deal with causation theory, as you know, and even more in philosophy of science. It’s a huge area and very important. However, no one’s views are dominant as far as I can tell, and none yet have ‘cashed out’ their theory in terms that would clarify how we should rehabilitate A and B to reduce their likelihood of re-offending. Indeed, individual B’s case implies that successful prevention might require rehabilitating the social/work context, not the person! Moreover, none of these has yet cashed out how to apply weights to causal vectors in a way relevant to prevention and intervention. We might think of genetic testing and gene therapy for A as a powerful prevention, and perhaps social constraints on shift work for B as a powerful prevention. Both are legitimate as could be other prevention strategies. Under Abrahamic FM assumptions, simply excusing A and charging/suing B is not a very effective or satisfying intervention for either party’s rehabilitation or prevention of future harms.
Then we also have the concept of ‘free will’ which Abrahamic FM assumptions depends upon and a serious consideration of complex causation in B’s case points to the many problems this concept poses when we start to understand complex networks of causal vectors. So an account of free will, or lack thereof, is needed.
Free will is a problematic notion for me for the purposes of adjudication and prevention of problem behaviors. I alluded to these in my prior essay for your ‘five ideas’ program. In short, I think that existing philosophical theories about free will are deficient in that I reject a common theme through all of them, namely, the concept of determinism, whether ‘strong’ or ‘weak’. The problem is that determinism marginalizes, or overlooks completely, the ever-present effects of entropy or randomness, which undermine deterministic accounts. I suspect this is why we don’t sue meteorologists for being wrong in weather predictions; randomness is a big limiting factor for their accuracy. What CMC-FM accounts need is an understanding of complex causality which includes the weight or causal power of randomness in particular situations. Hence my call for philosophers of science, mind, causality, psychiatry and so on! There’s work to be done!
Aftab: You recommend that “Criminology should partner with psychiatry as clinical psychology has done.” (p 508)
The clinical study and treatment of psychopathology is shared by medicine and psychology, but this partnership has also resulted in a broader notion of disorder, since in order for psychological treatments such as counseling and couple’s therapy to be reimbursed, disturbances of behavior have to be conceptualized as health problems. When it comes to rehabilitation of non-disordered immoral/criminal conduct, do you see the emergence of a sort of “clinical criminology” discipline? And if this discipline has a similar relationship to medicine as clinical psychology, do you think there will be a pressure to further expand the concept of healthcare to incorporate criminal rehabilitation?
Sadler: Your question moves farther ahead to a world that I hadn’t yet envisioned. Your question has some layers.
You mention that clinical psychology’s inclusion in mental health care has to do with needing reimbursement for ‘counseling’ and ‘couples therapy’. I don’t think the history of clinical psychology’s involvement with mental health care supports this formulation. A hundred years ago in the 20th century, progressive-era psychologists worked in asylums, state schools, and clinics alongside psychiatrists treating people with mental disorders that were historically prior to insurance reimbursement. The asylums used a team approach to mental health care then, much as we do now. American child psychiatry was founded to address the problem of juvenile delinquency, and psychologists and psychiatrists have argued for a hundred years about how to help intellectually disabled people. Medical insurance as we know it developed in the early 20th century Progressive era with pioneering companies like Blue Cross and Kaiser, ultimately leading to the first successful nationalized health insurance program in 1965—Medicare. Counseling preceded many biomedical treatments through mental health efforts like the moral therapy movement centuries before, beginning with Pinel. Modern ‘somatic’ treatments were relative latecomers. ‘Private practice’ grew out of mental health outpatient care in the mid-20th century. Importantly, what counts as a ‘disorder’ in the insurance era has more to do with economics and politics than the history of psychiatry and psychopathology proper. I would be confident in predicting, barring massive social change in the USA, that providing my kind of ‘rehabilitation’ for people with disorders of morality will still be mostly economic and political decisions, regardless of where psychiatry and philosophy stand. American psychiatry is still battling for equity in insurance coverage for plain old mental illnesses!
I could envision a clinical world where criminologists, with suitable training, could make substantive contributions in the mental health domain, most likely in care contexts where both disordered and ‘ordinary’ wrongful conduct is involved. What I had more in mind with your quote above is the more intermediate step of ‘forensic criminologists’ taking over the role of expert witnesses for criminal courts, instead of the current practice of forensic psychiatrists having this function. This was proposed as an intermediate step in an effort to take forensic psychiatry out of the role of contributing to the punishment of guilty defendants in our current system. In my view, this removes them from the morally dubious position of ‘doing harm’ through expert testimony rather than following our fundamental ethics of ‘do no harm.’ Readers of this article should know that the proposals I make for the future are staged in a loose, practical sequence having to do with feasible, easier changes done first, and more radical changes in psychiatry and criminal justice practice coming later. So the idea of forensic criminologists aiding courts as expert witnesses is something that has not developed much in the USA, but does have precedent and practice in Australia/New Zealand, which I write about in the book.
Aftab: You state that the boundaries of ordinary misconduct vs disordered misconduct should be treated similarly to the boundaries between ordinary and disordered anxiety, cognition, mood, and substance use. This ties in with a broader recognition of “morality as a psychological phenomenon” and disturbances of morality as a legitimate manifestation of psychopathology.
“[O]nce the exclusion of vice ‘experience’ is recognized and reversed, and the concept of disordered vice is admitted into the domain of medical psychopathology, a broad set of analogous philosophical tasks open up. Namely, these tasks involve sorting ordinary vice from pathological, disordered vice— the sorting out of particular conditions regarding their normal or pathological status.” (p 493)
One way of looking at the disorder/non-disorder distinction in psychopathology is that there is often a focus on whether the behavior in question is adaptive or maladaptive in terms of its functional impact, and there is often a focus on whether the behavior fulfils some evolutionary or biological function. Do you think there is a corresponding sense in which non-pathological vice can be considered adaptive and functional?
Sadler: Of course. I mention in the book the distinction between ‘kleptomania’ as vice-laden DSM disorder and ordinary shoplifting as a ‘non-pathological’ vice. If you are starving and broke, pocketing a sandwich in the store may be lifesaving. In an everyday sense, we make choices that from one perspective are vice-laden or wrongful that nonetheless might be construed from another viewpoint as valuable, functional, or adaptive. As familiar examples, consider all the TV and movies you’ve seen where the hero, or even the anti-hero, is confronted with dilemmas that require an assessment of higher- and lower-stakes in outcome. As a specific example, the detective who breaks the rules of police procedure in order to secure the greater good of capturing the bad guy. These moral rule-breakings fueled by greater-good assessments are something that all of us face, perhaps more often than we would like to admit. Moreover, in mental health care, particularly in psychotherapy, we often help our patients with analyses of greater-good actions—should I get a divorce, should I stay for the kids, are the kids better off with single parents than my spouse and I, etc. etc. In dialogue with the patient, the weighing and balancing of values and consequences around these kinds of decisions are the built-in practical ethics of mental health care. These decisions are also wrapped up in the complex-causal networks we discussed above. Regarding biological or evolutionary functions, I can’t comment on this in a scientifically justified way; evolutionary psychology is an area I have a lot of reservations about, but that’s another conversation.
Aftab: You make some radical proposals with regards to the practice of forensic psychiatry. In particular, you argue that under ideal circumstances the insanity defense should be abolished and that forensic psychiatry’s expert- witness role in criminal trials should end because this conflicts with the medical duty to serve the ill.
Some quotes:
“A nonpunitive, rehabilitative criminal justice system and criminal court obviates the need for an insanity defense.” (p 500)
“If we accept that criminal/ immoral conduct is subject to being disordered and criminal justice shifts toward nonpunitive rehabilitation and public protection, then the insanity defense debate disappears, as does the need for a differential social welfare response. If all antisocial conduct is subject to rehabilitation, then the silos of adult and juvenile criminal justice/ mental illness/ intellectual disability disappear and the focus on restoration of prosocial and healthy conduct becomes the overall goal for social welfare institutions.” (p 509)
“Forensic psychiatry’s expert- witness role in criminal trials should end (until a minimally punitive rehabilitative model is widespread).” (p 512)
“Forensic criminologists should replace psychiatric expert witnesses in criminal court proceedings… forensic criminologists, without a duty to serve the ill, can provide expert participation in criminal court process, allowing psychiatrists to maintain their loyalty to medical morality and adherence to the principle of ‘do no harm’. This aspirational/ ideal thesis requires much social change to implement. The training of such forensic criminologists will need to grow from a rare qualification to a standard, widespread one.” (p 513)
“The problematic sorting of categories of psychopathology eligible for, or not eligible for, NGRI defense should dissipate away because of irrelevance of NGRI to criminal justice rehabilitation.” (p 514)
Are there scholars within forensic psychiatry who have already made similar arguments? Are there forces within forensic psychiatry that are sympathetic to your vision?
Sadler: In the book I discuss Alan Stone’s critiques of forensic psychiatry from the 1980’s, as well as the critique from psychiatrists critical of expert testimony participation, particularly where the potential for death sentences is present. I also review the criticisms of Paul Appelbaum’s justifications for forensic participation in punitive court settings. These criticisms were co-articulated by one of the founders of the Association for the Advancement of Philosophy and Psychiatry and former APA President, Alfred Freedman. So the critique of forensic expert testimony in retributive justice settings is not new. What is novel to my work, I think, is the formulation that the paradoxes of forensic psychiatry emerge from the rivalry between two folk-metaphysical positions, where sometimes psychiatrists think in terms of personal responsibility, free will, individualism, and just deserts, and other times we think in terms of CMC folk-metaphysical assumptions. That’s why we have these seemingly arbitrary distinctions between mental disorders that are eligible for the insanity defense (such as schizophrenia) and ones that are not eligible in many, perhaps most, jurisdictions (such as pedophilic disorder). Implicit in these judgments are ideas like schizophrenia is more ‘innocent’ and pedophilic disorder is more ‘appalling’. On the court side, it’s also relevant to the legal criteria for the insanity defense, which vary from jurisdiction to jurisdiction, and even in some states where the insanity defense is not accepted by statute. Psychiatric culture jumbles up Abrahamic FM assumptions and CMC FM assumptions in a variety of ways.
Regarding what American and other forensic psychiatrists have to say about my work is yet to seen. A rewarding exception was the recent discussion of the book in Oxford at the Collaborating Centre for Values-Based Practice. I was privileged to have the book discussed by Phillip Candilis, a forensic psychiatrist and scholar based at St. Elizabeth’s Hospital in the DC area, and Rebecca Weintraub Brendel, a forensic psychiatrist and recent President of the American Psychiatric Association. At that meeting, both Candilis and Brendel acknowledged that my vision, while novel, may be very influential in the future and posed important challenges for the field in the years ahead. They both believed these ideas need to be considered carefully. However, I would be very surprised if this assessment was shared by the majority of U.S. forensic psychiatrists that go to the trouble to read Vice and Psychiatric Diagnosis. In the best of circumstances, the changes in forensic psychiatry I propose would be a massive hassle for them, and moreover, challenge long-held beliefs and assumptions about their field. I invite your readers to read the book and decide for themselves.
Aftab: You come out strongly in favor of rehabilitation rather than punishment- and vengeance-oriented retributive actions. “Instead of revenge and punishment we need scientific explanation, prevention, and effective rehabilitation strategies.” (p 507)
Where do we stand in terms of effectiveness of rehabilitative efforts at present. Do we have good evidence—e.g. in the form of randomized controlled trials—that rehabilitation is in fact successful in the real world and outperforms punitive measures?
Sadler: Yes, we have good evidence, but the challenge is in the quantity. The evidence of the efficacy of rehabilitative treatment for criminal conduct is discussed in various places in the book, but the most sustained discussion is in Chapter 8, section 8.5.2. There I describe the leading models of rehabilitation, the RNR model (Risk-Need-Responsivity model), as well as its cousin, the Good Lives model. I cite some of the studies, but more detail can be found in Bonta and Andrews’ now-sixth edition text, The Psychology of Criminal Conduct. Another great resource is Weisburd, Farrington, & Gill (2016).1
These models were a reaction to a culture of cynicism about the potential for criminal rehabilitation in the last quarter of the 20th century. They emerged in response to an influential article by sociologist Robert Martinson in 1974.2 Martin’s analysis contributed to a socio-political view that ‘nothing works’ in criminal rehabilitation, augmented by pop-culture tropes of the time (e.g., Clint Eastwood’s “Dirty Harry” cop, of “Go ahead punk, make my day” fame) and right-wing commentary of crime run amok. See a review in Cullen & Gendreau (2019).3 I should also mention the contemporary star of research into rehabilitation of the mentally ill offender, Jennifer L. Skeem, whose work can be viewed here.
As the stigma of offending carries gross deficiencies in research funding, the clinical-trial basis for these interventions remains small but promising. The RNR model is well established with its core of cognitive-behavioral treatment and development of prosocial behaviors, as well as with their well-validated assessment instruments, but the studies are small in size and things like comparative effectiveness trials are just not there yet.
This work should be considered, however, in the context of the research on the toxic effect of retributive justice/punishment, where the triad of traumatic incarceration, peer socialization of antisocial skills (hardening), and withholding of post-release social support contributes to increased risks of re-offending. Perhaps the champion of this critique is Gregg Caruso; see his review: Caruso (2021).4 Regarding the ‘real world’ stipulation: if your social policy sets up people to fail, then, not surprisingly, they tend to fail.
Aftab: Your discussion of vice in psychopathology is also quite relevant for dimensional classifications and the presence of vice-laden phenomena in HiTOP in some ways is already a demonstration that disturbances of moral conduct can indeed be based on the same logic as other disorders.
Aftab:
“DSM- style and other categories of mental disorder of the future should consider moral conduct as a relevant mental function like cognition, conation, and affection, and be subject to disorder status based on the same conceptual and empirical criteria as the other, nonmoral mental disorders.” (p 507)
It is unclear what the scientific future of DSM-style categories is. There has been a massive turn towards dimensional classifications in recent years. I am myself engaged with the HiTOP literature these days. The presence of vice-laden behavior is quite evident in the Externalizing superspectrum in the model, and vice-laden symptoms and traits form homogenous factors such as “Disinhibition” and “Antagonism,” similar to psychopathological phenomena in the Internalizing spectrum. So, your discussion of vice in psychopathology is also quite relevant for dimensional classifications and the presence of vice-laden phenomena in HiTOP in some ways is already a demonstration that disturbances of moral conduct can indeed be based on the same logic as other disorders. Any thoughts?
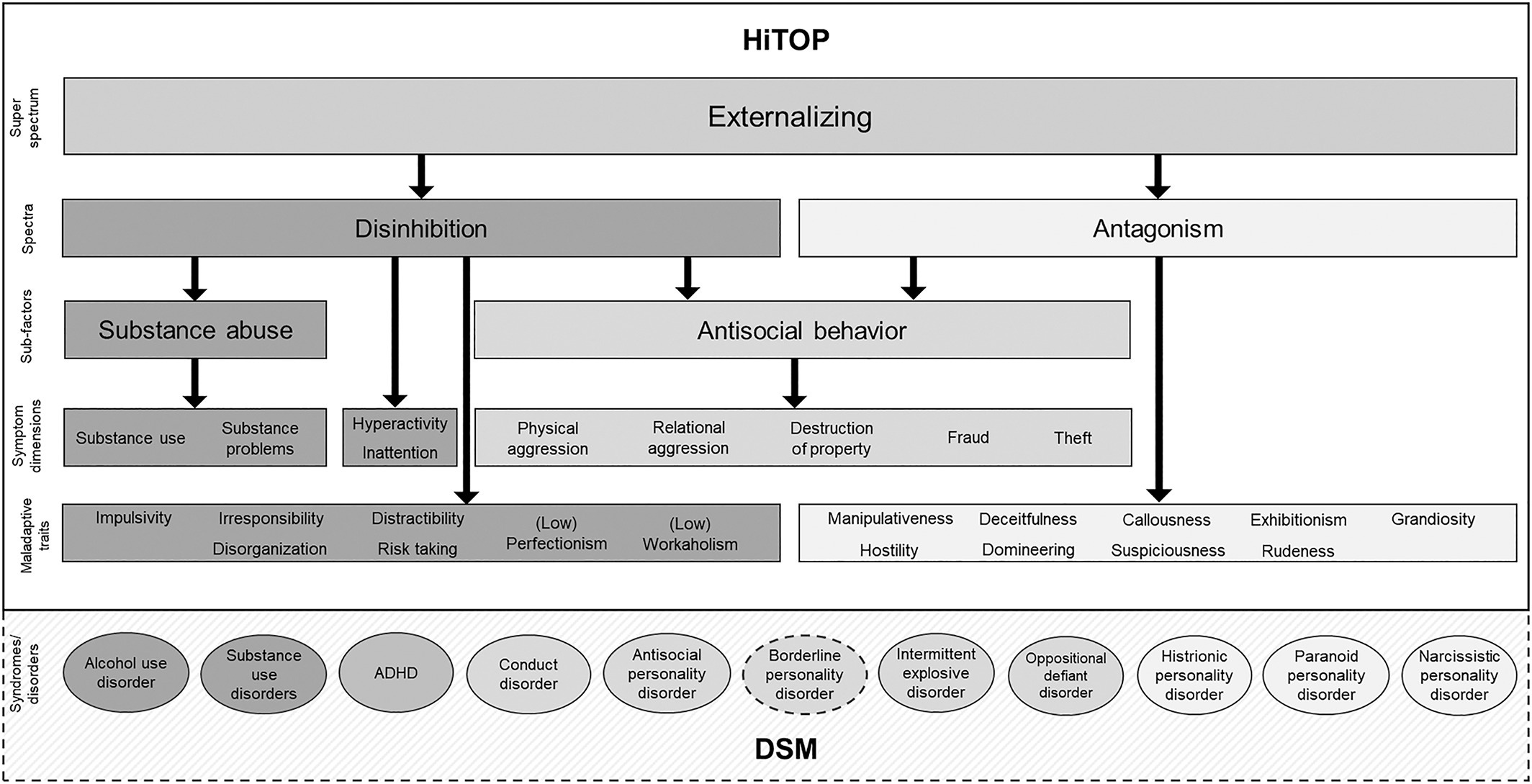
Sadler: I generally avoid soothsaying, being wrong way too often, so I don’t know what will happen to the DSMs and the APA’s hold on psychiatric classification. The HiTOP figure though is very interesting. As you note, this is another example of how vice-laden concepts can be integrated into mental health/illness research. Your response here is exactly the kind of next-step synthesis I was hoping to inspire. Dr. Aftab, you should write more on this!
Aftab: Thank you!
This post is part of a series featuring interviews and discussions intended to foster a re-examination of philosophical and scientific debates in the psy-sciences. See prior discussions here.
See also:

Weisburd, D., Farrington, D. P., & Gill, C. (Eds.). (2016). What works in crime prevention and rehabilitation: Lessons from systematic reviews.
Martinson, R. 1974. What works? Questions and answers about prison reform. The Public Interest, 35(2), 22-54.
Cullen, F. T., & Gendreau, P. (2019). From nothing works to what works: Changing professional ideology in the 21st century. In Clinical forensic psychology and law (pp. 231-256)
Caruso, G. D. (2021). Rejecting retributivism: free will, punishment, and criminal justice. Cambridge University Press
I wrote my doctoral dissertation on free will. I published mostly on free will and moral responsibility in the more abstract sense before going into psych stuff. I still teach free will. But I don't understand what this part means:
"Free will is a problematic notion for me for the purposes of adjudication and prevention of problem behaviors. I alluded to these in my prior essay for your ‘five ideas’ program. In short, I think that existing philosophical theories about free will are deficient in that I reject a common theme through all of them, namely, the concept of determinism, whether ‘strong’ or ‘weak’. The problem is that determinism marginalizes, or overlooks completely, the ever-present effects of entropy or randomness, which undermine deterministic accounts."
Maybe there's some mix-up here between how philosophers use the term "determinism" and how it may be used outside of our field?
Carl Hoefer defines determinism as follows at the Stanford Encyclopedia of Philosophy:
"Determinism: Determinism is true of the world if and only if, given a specified way things are at a time t, the way things go thereafter is fixed as a matter of natural law."
We don't know if the world is deterministic in this sense. Arguably, quantum mechanics suggests that it's not. But it MIGHT be deterministic in this sense and yet, quite often, impossible to predict for mere mortals. The weather may be too chaotic to ever predict, human behaviour may be too complicated to ever predict, the behaviour of elementary particles may be impossible to predict even if they ultimately obey some deep deterministic laws that we don't know about, etc. All of this could be true even if the universe is ultimately deterministic.
Philosophers discuss what, if anything, follows if the world is deterministic, but few people would say with any confidence that it IS (you have an easier time finding free will philosophers who say with any confidence that it's probably NOT).
But, John and Awais, if you wanna read up on free will, moral responsibility and retributivism, COME TO ME! I have the papers!
I've argued that debates about free will and moral responsibility will likely go on forever in philosophy, because you've got several camps whose theories are compatible with our best science but differ in which intuitions they rely on. Most likely, people's intuitions are just different, and will never homogenize, so we'll always have these different camps.
But that in itself is a reason not to have a retributivist criminal justice system. It's as illiberal to base a societal institution on controversial philosophical theories, built on intuitions that not everyone shares, as it would be to base it on some religion that not everyone shares. https://link.springer.com/article/10.1007/s12152-020-09436-6
Here, I defend my own brand of compatibilism: https://link.springer.com/article/10.1007/s11098-019-01292-2 I believe I'm right and philosophers who disagree with me are wrong. But I would never stake someone's life or liberty on that claim!
And here's a madness/psych-oriented paper about moral responsibility, where I discuss how it's unfeasible AND undesirable to try to replace what you call "folk-psychology" here completely with causal explanations of behaviour. https://imsj.journals.publicknowledgeproject.org/index.php/imsj/article/view/5243
Here, I argue that it's often better to focus on external obstacles that people face than either brain dysfunctions or philosophical free will scepticism if you want to excuse them: https://onlinelibrary.wiley.com/doi/10.1111/phis.12243
This isn't all, of course! I've got tons! You wanna learn more about free will and moral responsibility and how to fit them within a scientific worldview, I've got your backs!
The way I heard the maxim is: “T'is hell to write, but heaven to have written." Ironically, I heard this the very day I finished my doctoral dissertation from a perfect stranger while doing some photocopying in the university library.
Please consider a possible error:
"After my talk at the International Network for Philosophy and Psychiatry meeting *last year* in Vienna, Diogo came up to me and recited chapter and verse from VAPD2 about how I had problematized the issue of ‘vice-laden disorders’ in that book."
If this encounter happened last year, how could Diogo be quoting from VAPD2?
We historians are sensitive to chronology.